


Alcohol affects the brain by disrupting the balance between two key neurotransmitter systems, the GABA activity and the excitatory glutamate signaling.
Alcohol amplifies inhibitory GABA activity while suppressing excitatory glutamate signaling, producing the sedation, impaired coordination, and cognitive blunting that define intoxication. These acute effects reverse when alcohol clears, but repeated heavy exposure causes structural and functional brain changes that persist long after drinking stops.
Understanding exactly how alcohol affects the brain clarifies why alcohol use disorder is a neurological condition, not a failure of willpower.
Key Takeaways
- Alcohol acts as a positive allosteric modulator of GABA-A receptors and a competitive antagonist at NMDA glutamate receptors, simultaneously depressing neural excitation and enhancing inhibition.
- According to the National Institute on Alcohol Abuse and Alcoholism (NIAAA), heavy alcohol use is associated with a 10% reduction in brain volume in regions including the prefrontal cortex, hippocampus, and cerebellum.
- Long-term alcohol use disorder is linked to Wernicke-Korsakoff syndrome, a thiamine deficiency-driven neurological emergency characterized by ataxia, ophthalmoplegia, and severe anterograde amnesia.
- Short-term alcohol effects on the brain are dose-dependent and progress from mild impairment at low blood alcohol concentrations to life-threatening respiratory depression at BAC levels above 0.30%.
- The brain demonstrates neuroplastic recovery after alcohol cessation, with structural improvements documented in multiple regions following sustained abstinence, though some damage may be permanent.
How Alcohol Affects the Brain: The Core Mechanism
Alcohol is not a simple central nervous system (CNS) depressant. It exerts complex, dose-dependent effects across multiple neurotransmitter systems simultaneously.
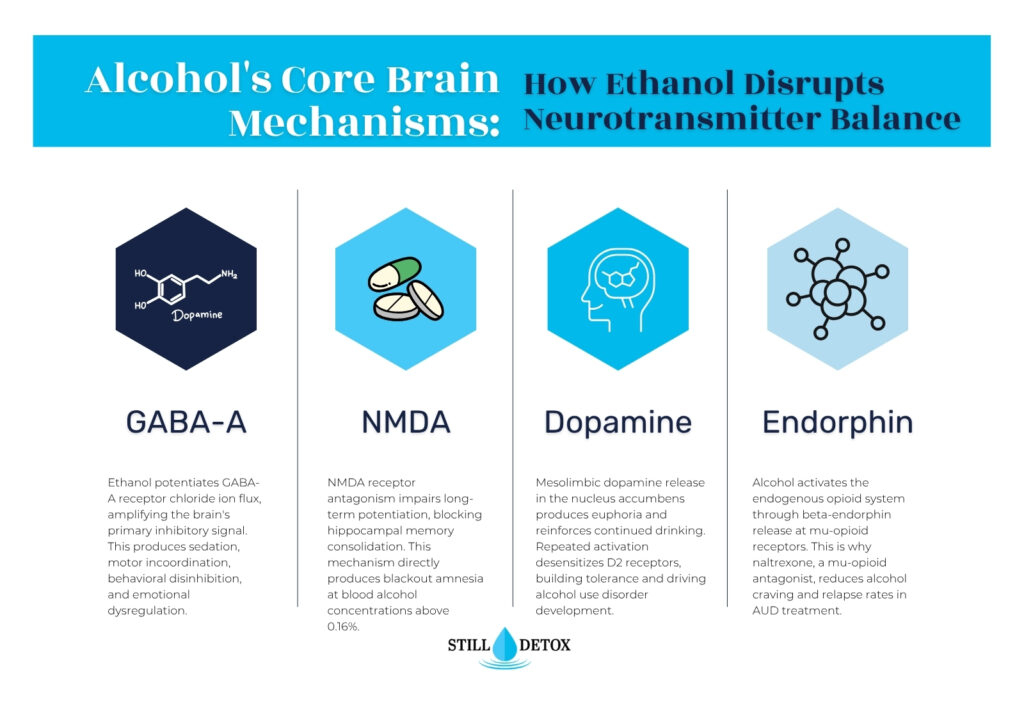
At the molecular level, ethanol potentiates GABA-A receptor chloride ion flux, amplifying the brain’s primary inhibitory signal. GABA-A receptor activation hyperpolarizes neurons by increasing intracellular chloride concentration, reducing their likelihood of firing. Ethanol’s GABA-A modulation is particularly pronounced in the cerebellum, brainstem, and limbic system, accounting for the motor incoordination, behavioral disinhibition, and emotional dysregulation observed during intoxication.
Simultaneously, ethanol antagonizes NMDA glutamate receptors, the brain’s primary excitatory receptor subtype. NMDA receptor blockade impairs long-term potentiation (LTP), the synaptic process underlying memory consolidation. This mechanism directly produces the anterograde amnesia and “blackout” phenomena associated with acute intoxication.
Dopamine and the Reinforcement Loop
Alcohol stimulates dopamine release in the nucleus accumbens, the brain’s primary reward center. This dopaminergic surge produces the euphoria, relaxation, and social disinhibition that reinforce continued drinking. Repeated alcohol-induced dopamine release progressively desensitizes dopamine D2 receptors, requiring escalating alcohol quantities to achieve the same rewarding effect. This tolerance-building process is a core mechanism in the neurobiological development of alcohol use disorder (AUD).
Endogenous Opioid System Activation
Alcohol activates the endogenous opioid system by stimulating the release of beta-endorphin, an endogenous opioid peptide that binds mu-opioid receptors in the mesolimbic pathway. This opioid activation contributes to the euphoric and anxiolytic effects of alcohol and explains why naltrexone, a mu-opioid receptor antagonist, reduces alcohol craving and relapse rates in AUD treatment.
Short-Term Effects of Alcohol on the Brain: Stages of Intoxication
Alcohol’s short-term effects on the brain follow a dose-dependent progression determined primarily by blood alcohol concentration (BAC). The pattern below reflects typical effects in an average adult without significant alcohol tolerance.
- BAC 0.02 to 0.05% (1 to 2 standard drinks): Mild euphoria and lowered inhibitions as prefrontal cortex suppression reduces judgment and impulse control. Reaction time begins to slow. Social confidence increases from limbic system disinhibition.
- BAC 0.06 to 0.10% (2 to 4 standard drinks): Impaired coordination and judgment as cerebellar GABA-A modulation disrupts fine motor control. Memory encoding begins to falter. Emotional reactivity increases as the amygdala becomes disinhibited.
- BAC 0.11 to 0.15% (4 to 6 standard drinks): Slurred speech, significant cognitive impairment, and emotional instability as widespread cortical suppression deepens. Balance and gait are clearly impaired. Nausea can emerge from brainstem stimulation.
- BAC 0.16 to 0.25% (6 to 10 standard drinks): Blackout risk as NMDA receptor blockade sufficiently suppresses hippocampal LTP to prevent memory consolidation. Motor control is severely compromised. Vomiting reflex may be impaired, increasing aspiration risk.
- BAC 0.25% and above: Life-threatening CNS depression as brainstem respiratory and cardiovascular centers are suppressed. Unconsciousness, respiratory depression, and death become possible without emergency intervention.
Long-Term Effects of Alcohol on the Brain
Structural Brain Changes from Chronic Alcohol Use
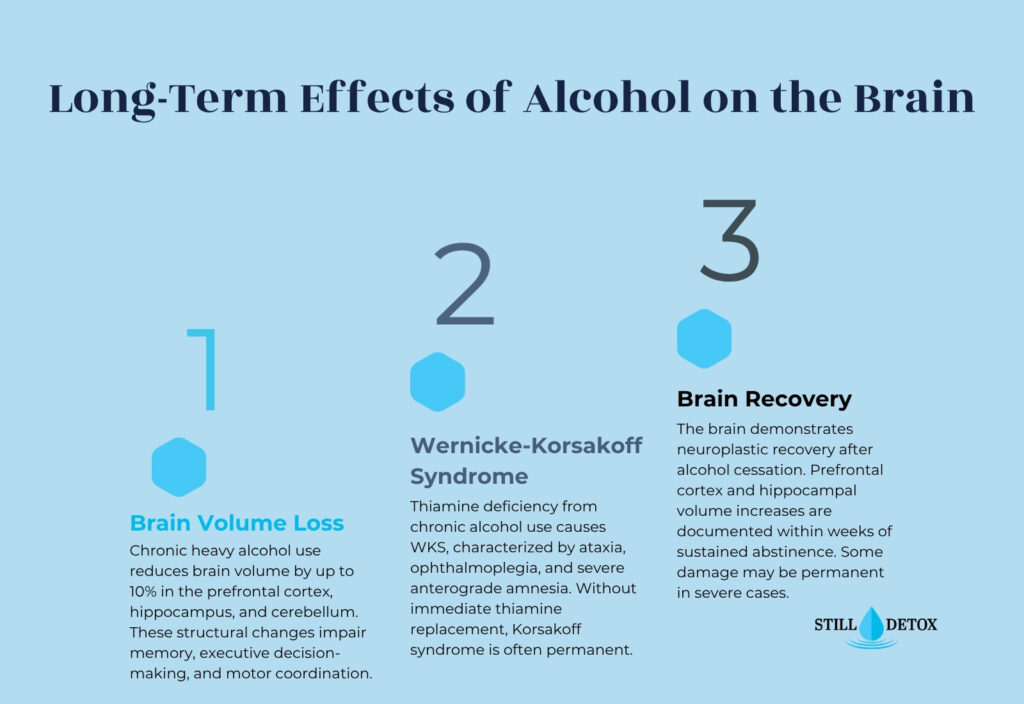
Chronic heavy alcohol consumption causes measurable volumetric reductions across multiple brain regions. The prefrontal cortex, hippocampus, and cerebellum demonstrate the most consistent shrinkage in neuroimaging studies of individuals with long-term alcohol use disorder. According to the NIAAA, heavy drinking is associated with up to 10% global reduction in brain volume.
Prefrontal cortex atrophy impairs executive function, decision-making, and impulse control. This structural change creates a neurobiological feedback loop: frontal lobe damage reduces the capacity to evaluate consequences of drinking, which sustains drinking behavior despite mounting harm. Hippocampal volume loss impairs explicit memory formation and spatial navigation, producing the memory deficits that characterize AUD.
Wernicke-Korsakoff Syndrome
Wernicke-Korsakoff syndrome (WKS) is a severe neurological complication of chronic alcohol use driven by thiamine (vitamin B1) deficiency. Alcohol impairs thiamine absorption, increases thiamine metabolic demand, and reduces hepatic thiamine storage simultaneously.
WKS presents in two phases. Wernicke encephalopathy is the acute phase, characterized by a classic triad of ataxia, ophthalmoplegia (abnormal eye movements), and acute confusional state. Without immediate thiamine replacement, Wernicke encephalopathy progresses to Korsakoff syndrome, which is characterized by severe anterograde amnesia (inability to form new memories), retrograde amnesia covering years prior to illness, and confabulation (unconscious fabrication of false memories). Korsakoff syndrome is often permanent.
Alcoholic Neuropathy
Chronic alcohol use disorder causes alcoholic neuropathy through both direct ethanol neurotoxicity and nutritional deficiencies, particularly B-vitamin depletion. Alcoholic neuropathy presents as symmetrical peripheral neuropathy: numbness, burning pain, and weakness beginning in the feet and progressing proximally. Unlike Wernicke-Korsakoff syndrome, alcoholic neuropathy reflects both central and peripheral nervous system damage.
Alcohol-Related Brain Damage and Dementia
Chronic alcohol use is an independent risk factor for alcohol-related dementia (ARD), characterized by progressive cognitive decline across executive function, memory, processing speed, and visuospatial domains. ARD is pathologically distinct from Alzheimer’s disease but shares the clinical presentation of significant cognitive impairment in daily functioning. According to the DSM-5-TR, alcohol-induced major neurocognitive disorder applies when cognitive decline exceeds expected effects of intoxication or withdrawal and persists beyond 60 days of abstinence.
What Are the 5 Effects of Alcohol on the Brain?
The five most clinically significant effects of alcohol on the brain are:
- 1. GABA-A potentiation: Produces sedation, motor incoordination, and anxiolysis at acute doses.
- 2. NMDA antagonism: Impairs memory consolidation, produces blackout amnesia, and suppresses neural excitation.
- 3. Dopaminergic activation: Generates euphoria, reinforces drinking behavior, and drives the development of tolerance.
- 4. Prefrontal cortex suppression: Impairs executive function, judgment, and impulse control during intoxication and, with chronic use, structurally.
- 5. Neurotoxic atrophy: Chronic exposure reduces brain volume in prefrontal cortex, hippocampus, and cerebellum, impairing memory, decision-making, and motor coordination permanently in severe cases.
Does the Brain Recover from Alcohol Use Disorder?
The brain demonstrates significant neuroplastic capacity following alcohol cessation. Neuroimaging studies document volumetric recovery in the prefrontal cortex and hippocampus beginning within weeks of sustained abstinence. Gray matter density increases in multiple cortical regions during the first year of sobriety, with measurable functional improvements in working memory, executive function, and processing speed.
Recovery is not uniform or complete in all cases. Wernicke-Korsakoff syndrome produces permanent amnestic damage in the majority of cases, particularly when thiamine replacement was delayed. Alcoholic neuropathy partially reverses with abstinence and nutritional rehabilitation but may not fully resolve in individuals with severe, long-standing damage. The extent of brain recovery depends on the duration of heavy drinking, age at which heavy use began, severity of nutritional deficiencies, and presence of co-occurring medical conditions.
What Are Signs of Alcohol-Related Brain Damage?
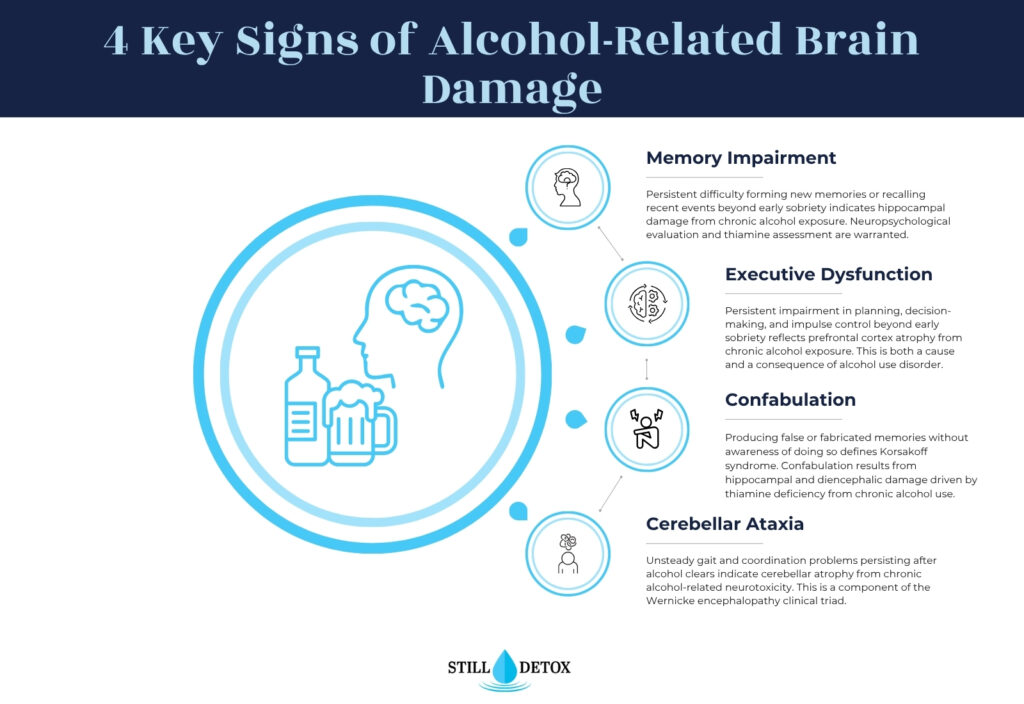
Signs that alcohol-related brain damage may have occurred include:
- Persistent memory impairment: Difficulty forming new memories or recalling recent events after prolonged abstinence.
- Executive dysfunction: Persistent difficulty planning, organizing, or managing impulse control beyond expected early sobriety cognitive fog.
- Gait or balance abnormalities: Unsteady walking or coordination problems that persist after alcohol clears and are not explained by other causes.
- Confabulation: Producing false or fabricated memories without awareness of doing so.
- Word-finding difficulties: Persistent anomia or expressive language impairment beyond early recovery.
Any of these signs warrant neuropsychological evaluation and thiamine status assessment.
Alcohol Use Disorder Treatment at Still Detox
Addressing alcohol’s effects on the brain requires medical supervision during withdrawal and structured therapeutic support during recovery. Alcohol withdrawal can be life-threatening, and professional detox is the appropriate first intervention.
Medical Detox for Alcohol Withdrawal
Still Detox’s medically supervised detox program addresses the neurological rebound that occurs when GABA-A and NMDA systems adapt to alcohol’s absence. Alcohol withdrawal syndrome produces neural hyperactivity driven by GABA deficiency and NMDA receptor upregulation, manifesting as tremors, anxiety, hypertension, and in severe cases, grand mal seizures and delirium tremens. Clinical monitoring using validated tools such as the CIWA-Ar (Clinical Institute Withdrawal Assessment for Alcohol) guides medication protocols during detox. Same-day medical assessment is available.
Residential Treatment
Still Detox’s residential program provides structured evidence-based therapy targeting the cognitive and behavioral patterns of alcohol use disorder. Cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT) address the executive dysfunction and emotional dysregulation that both contribute to and result from chronic alcohol exposure.
Dual Diagnosis Treatment
Co-occurring anxiety disorders, major depressive disorder, and post-traumatic stress disorder frequently co-occur with alcohol use disorder. Still Detox’s integrated dual diagnosis approach treats both conditions simultaneously, addressing the neurochemical overlap between AUD and co-occurring psychiatric presentations.
Frequently Asked Questions
What are the 5 effects of alcohol on the brain?
Alcohol’s five primary brain effects are GABA-A receptor potentiation (sedation and motor impairment), NMDA receptor antagonism (memory blackout and excitatory suppression), mesolimbic dopamine activation (euphoria and reinforcement), prefrontal cortex suppression (impaired judgment and impulse control), and neurotoxic structural atrophy with chronic heavy use affecting the prefrontal cortex, hippocampus, and cerebellum.
What are the 7 stages of being drunk?
Intoxication progresses through approximately seven stages based on BAC: sobriety (below 0.02%), euphoria (0.03 to 0.12%), excitement (0.09 to 0.25%), confusion (0.18 to 0.30%), stupor (0.25 to 0.40%), coma (0.35 to 0.50%), and death (above 0.45%). Individual variation in tolerance and body weight shifts these thresholds significantly. These stages reflect progressive CNS depression across brainstem, cerebellar, and cortical systems.
Does your brain ever recover from alcohol?
Yes, the brain demonstrates documented neuroplastic recovery following alcohol cessation. Volumetric imaging studies show prefrontal cortex and hippocampal gray matter recovery beginning within weeks of sustained abstinence, with functional improvements in memory and executive function documented over the first year of sobriety. Recovery is partial in cases involving Wernicke-Korsakoff syndrome, severe alcoholic neuropathy, or prolonged heavy use beginning in adolescence, where some damage may be permanent.
What are signs of brain damage from alcohol?
Signs of alcohol-related brain damage include persistent memory impairment beyond early sobriety, executive dysfunction, gait or balance abnormalities without other explanation, confabulation (producing false memories without awareness), and word-finding difficulties. Wernicke-Korsakoff syndrome specifically presents with the triad of ataxia, ophthalmoplegia, and acute confusional state. Any of these findings after prolonged abstinence warrant neuropsychological evaluation and medical workup.
References
- National Institute on Alcohol Abuse and Alcoholism. (2024). Alcohol’s Effects on the Body. https://www.niaaa.nih.gov/alcohols-effects-health/alcohols-effects-body
- National Institute on Drug Abuse. (2023). Alcohol DrugFacts. https://nida.nih.gov/publications/drugfacts/alcohol
- National Institute on Alcohol Abuse and Alcoholism. (2023). Wernicke-Korsakoff Syndrome. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/wernicke-korsakoff-syndrome
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR).
- Cleveland Clinic. (2024). Alcohol Use Disorder.
- Oscar-Berman, M., & Marinković, K. (2007). Alcohol: Effects on neurobehavioral functions and the brain. Neuropsychology Review, 17(3), 239–257.


