


Relapse means a return to substance use after a period of abstinence.
In clinical terms, relapse is not a sudden event but a progressive process that unfolds across emotional, mental, and physical stages before active substance use resumes. Understanding what relapse means and what precedes it is essential to interrupting the cycle before it completes.
Relapse is common in recovery. It signals that a dimension of treatment needs strengthening, not that recovery has permanently failed.
Key Takeaways
- Relapse is defined clinically as a return to substance use following a period of abstinence and represents a predictable risk in the course of any substance use disorder, not an endpoint.
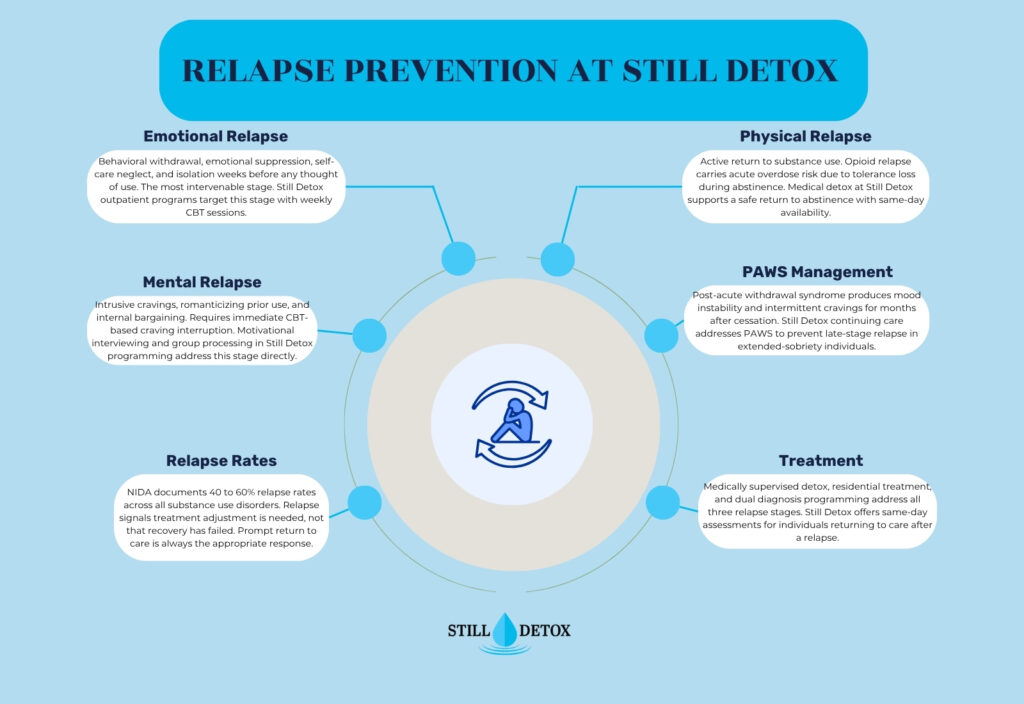
- According to the National Institute on Drug Abuse (NIDA), relapse rates for substance use disorders range from 40 to 60%, comparable to relapse rates for other chronic medical conditions including hypertension and type 2 diabetes.
- Relapse occurs in three recognized stages: emotional relapse, mental relapse, and physical relapse. Most relapse prevention interventions target the emotional stage, which begins weeks before active use.
- High-risk relapse triggers include unmanaged stress, social isolation, environmental cues associated with prior use, co-occurring untreated mental health conditions, and post-acute withdrawal syndrome (PAWS).
- Returning to treatment immediately after a relapse significantly reduces long-term harm, particularly for opioid use disorder where tolerance loss during abstinence sharply increases overdose fatality risk.
What Does Relapse Mean?
In clinical addiction medicine and the DSM-5-TR framework, relapse refers to a return to substance use following a period of intentional abstinence in the course of treating a substance use disorder. The term applies across all substance use disorder diagnoses, including alcohol use disorder (AUD), opioid use disorder (OUD), stimulant use disorder, and cannabis use disorder.
Relapse is distinct from a lapse. A lapse is a single, isolated instance of substance use that does not escalate into a pattern. A relapse describes a sustained return to problematic use patterns. This distinction matters clinically because intervention strategy differs: a lapse may be managed with immediate outreach and coping skill reinforcement, while a relapse typically requires a return to structured treatment.
Is Relapse a Sign of Treatment Failure?
Relapse is a predictable feature of chronic disease management, not evidence of treatment failure or moral weakness. NIDA explicitly frames relapse in substance use disorder as analogous to a missed medication dose or dietary deviation in conditions like hypertension or type 2 diabetes. The presence of relapse indicates that treatment intensity or focus needs adjustment, not that the individual is incapable of recovery.
What Does Relapse Mean on TikTok and in Everyday Language?
The term relapse is used colloquially on social media platforms including TikTok to describe returning to any unwanted habit or behavior, including emotional struggles, disordered eating patterns, or self-harm behaviors. In behavioral health and addiction medicine, the term retains its specific clinical meaning: a return to substance use following abstinence. When encountering relapse language in informal contexts, it is important to distinguish between colloquial and clinical usage, as the implications and appropriate responses differ significantly.
The Three Types of Relapse
Emotional Relapse
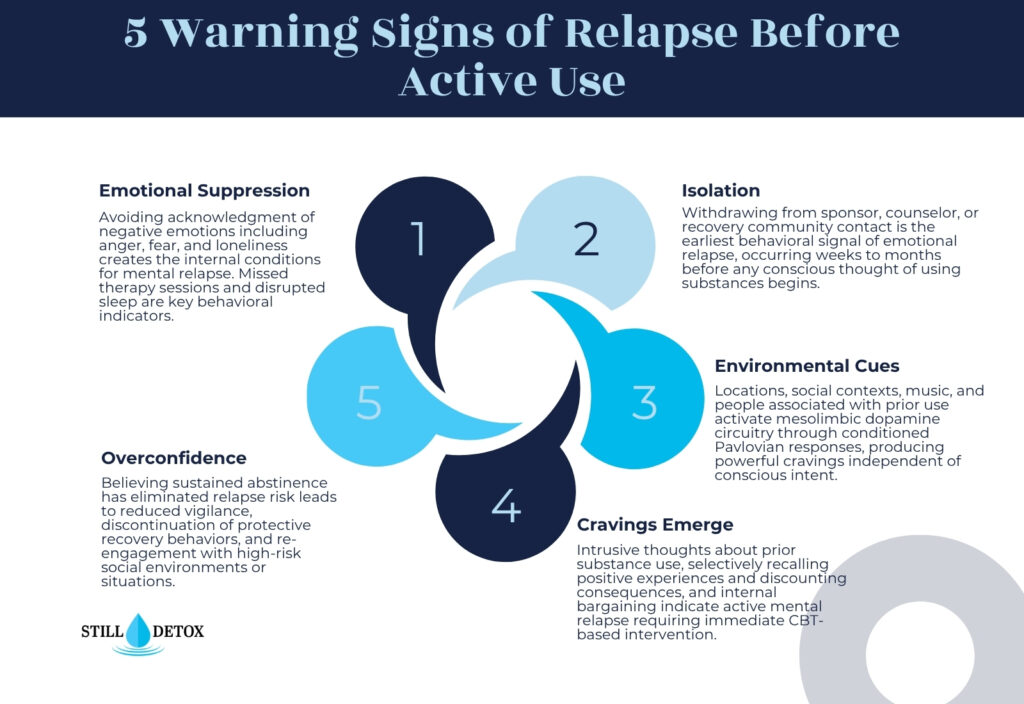
Emotional relapse is the first stage and begins weeks or months before any thought of using substances. During emotional relapse, the individual is not consciously thinking about using, but their behavior and emotional state are creating the conditions that make use likely.
Signs of emotional relapse include:
- Isolating from support networks: Withdrawing from sponsor, counselor, or recovery community contact.
- Suppressing emotions: Avoiding acknowledging or processing negative feelings, particularly anger, fear, and loneliness.
- Neglecting self-care: Disrupted sleep patterns, skipped meals, missed therapy sessions, and abandonment of recovery routine.
- Attending support meetings without participating: Physical presence without emotional engagement or honest self-disclosure.
Emotional relapse is the most intervenable stage. Identifying and addressing these warning behaviors before mental relapse begins is the primary goal of relapse prevention planning.
Mental Relapse
Mental relapse involves an internal conflict between recovery intentions and thoughts about using. The individual begins experiencing urges and actively entertaining the idea of using, often with increasing intensity over time.
Signs of mental relapse include:
- Cravings: Intrusive thoughts about the substance, the experience of using, or locations associated with past use.
- Romanticizing prior use: Selectively recalling positive aspects of substance use while discounting consequences.
- Bargaining: Rationalizing that controlled or occasional use is now possible (“I’ve been clean long enough that I can handle one drink”).
- Planning around use: Structuring activities or schedules to create opportunity for use without detection.
Mental relapse requires active therapeutic intervention, including craving interruption techniques from cognitive behavioral therapy (CBT), contact with a counselor or sponsor, and honest disclosure of urges within the recovery support network.
Physical Relapse
Physical relapse is the stage at which substance use actually occurs. It begins with a lapse, the first instance of use, which rapidly escalates to full return of prior use patterns in many individuals due to the neurobiological sensitization of reward pathways that occurred during active addiction.
Physical relapse carries acute medical risks beyond the psychological consequences of returning to use. Individuals who relapse on opioids after a period of abstinence face sharply elevated overdose fatality risk because tolerance to opioid respiratory depression diminishes during abstinence. Returning to a previously used dose after a period of opioid abstinence can produce fatal respiratory depression at a dose that was previously tolerated without incident.
What Causes Relapse?
Common Relapse Triggers
Relapse triggers are internal or external stimuli that activate craving and drug-seeking behavior through conditioned learning mechanisms. The most evidence-supported relapse triggers include:
- Stress: Corticotropin-releasing factor (CRF) released during stress activates the extended amygdala, which drives negative reinforcement-based substance seeking. Unmanaged acute stress is the most consistently identified relapse precipitant across all substance use disorders.
- Environmental cues: Locations, social contexts, music, smells, and people associated with prior use activate mesolimbic dopamine circuitry through conditioned Pavlovian responses, producing powerful cravings independent of conscious intent.
- Social pressure: Direct offers to use or social environments where substance use occurs create both access and normative pressure.
- Negative emotional states: Anxiety, depression, loneliness, and anger drive relapse through negative reinforcement pathways when emotional regulation skills are insufficient.
- Overconfidence: Believing that sustained abstinence has eliminated relapse risk leads to reduced vigilance and discontinuation of protective recovery behaviors.
Post-Acute Withdrawal Syndrome (PAWS) as a Relapse Driver
Post-acute withdrawal syndrome (PAWS) is a prolonged neuroadaptation period following acute withdrawal that can persist for months to years. PAWS produces symptoms including mood instability, cognitive fog, sleep disruption, and intermittent cravings that fluctuate without obvious triggering events. PAWS is particularly pronounced following alcohol and benzodiazepine cessation and is a significant but under-recognized driver of late-stage relapse in individuals who have achieved extended sobriety.
Co-Occurring Mental Health Conditions
Untreated co-occurring disorders including major depressive disorder, generalized anxiety disorder, PTSD, and bipolar disorder dramatically increase relapse risk. Substance use often begins as self-medication for psychiatric symptoms, and when those symptoms return or intensify during abstinence without treatment, the neurobiological pull toward substance use as emotional relief intensifies correspondingly.
What to Do After a Relapse
Immediate Safety Steps
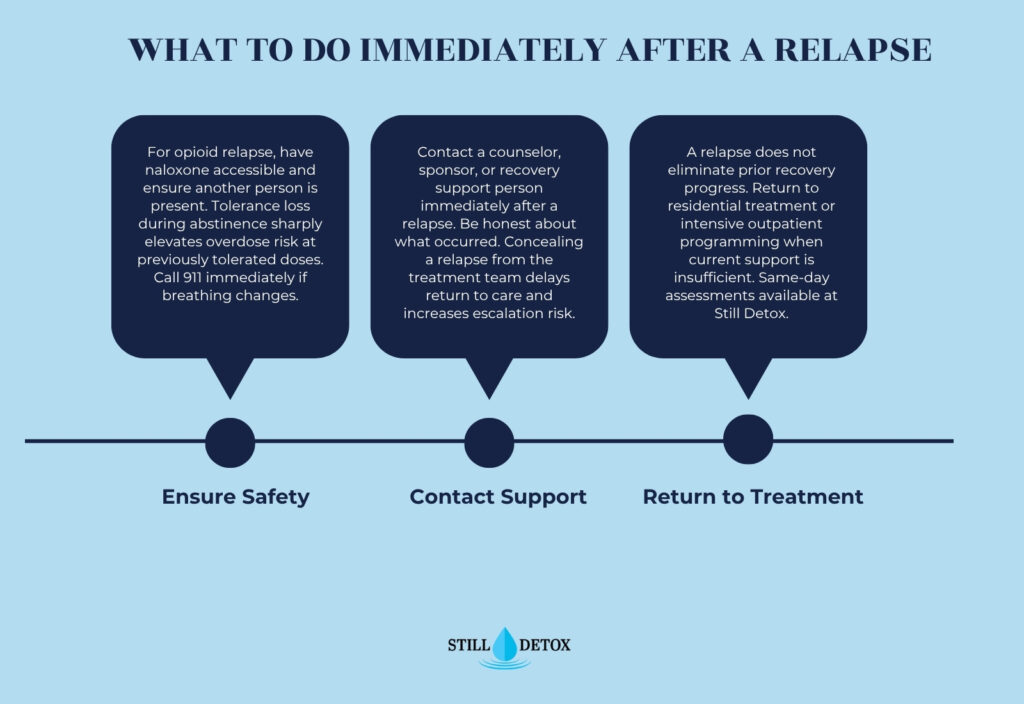
A relapse does not eliminate prior recovery progress. The most important immediate action is ensuring physical safety and preventing escalation of use. For opioid relapse specifically, every episode carries overdose risk. The following steps apply immediately after a relapse occurs:
- Ensure physical safety first: If an opioid was used after a period of abstinence, have naloxone (Narcan) accessible and ensure another person is present. Call emergency services immediately if breathing changes.
- Do not continue using: Stopping after a lapse prevents progression to full relapse.
- Contact a counselor, sponsor, or recovery support person immediately.
- Be honest: Concealing a relapse from the treatment team delays return to care and increases risk.
When to Return to Treatment
Returning to a higher level of care is often the appropriate response to relapse. A relapse does not mean starting over from nothing. It means the current support level needs adjustment. Residential treatment, intensive outpatient programming, or stepped-up individual therapy are all appropriate depending on the severity of the relapse and the individual’s current circumstances.
Relapse Prevention and Treatment at Still Detox
Relapse prevention is a core competency of every level of care at Still Detox. Addressing the emotional, cognitive, and neurobiological dimensions of relapse risk is integrated throughout the treatment continuum.
Medical Detox for Return to Care
For individuals returning to treatment following a physical relapse involving alcohol or opioids, medical detox provides supervised support through withdrawal. Still Detox’s medical team initiates the CIWA-Ar or COWS clinical assessment protocols on arrival and adjusts care based on the severity of re-emergent withdrawal. Same-day assessment is available for individuals in acute relapse.
Residential Treatment with Relapse-Informed Programming
Still Detox’s residential program incorporates structured relapse prevention therapy, targeting the emotional and mental relapse stages through cognitive behavioral therapy, motivational interviewing, and daily group processing of triggers and cravings. Treatment planning after a relapse specifically addresses the circumstances that preceded the return to use.
Dual Diagnosis Treatment
Co-occurring psychiatric conditions that drive relapse are addressed within Still Detox’s integrated dual diagnosis model. Treating depression, anxiety, PTSD, and other co-occurring conditions reduces the neurobiological pressure toward substance use as self-medication.
Frequently Asked Questions
What does relapse mean on TikTok?
On TikTok and social media broadly, relapse is used colloquially to describe returning to any unwanted behavior, not exclusively substance use. In clinical behavioral health terms, relapse specifically describes a return to substance use following abstinence in the course of treating a substance use disorder. The social media usage is informal and covers a wide range of behaviors not addressed by the clinical definition.
What is the meaning of the word relapse?
Relapse derives from the Latin relabi, meaning “to slip back.” In medicine and addiction treatment, it describes a return to a previous condition after a period of improvement. In the substance use disorder context, relapse means returning to substance use after a period of intentional abstinence and represents a recognized stage in the course of a chronic, treatable condition.
Is relapse good or bad?
Relapse is neither a moral good nor an endpoint of recovery. Clinically, relapse indicates that the current treatment approach, support structure, or coping resources need strengthening. NIDA documents relapse rates of 40 to 60% for substance use disorders, comparable to other chronic medical conditions. Responding promptly to a relapse by returning to professional treatment reduces long-term harm and sustains the overall trajectory toward recovery.
What are the three types of relapse?
The three clinically recognized stages of relapse are emotional relapse (behavioral withdrawal, emotional suppression, self-care neglect, weeks to months before use), mental relapse (intrusive cravings, romanticizing prior use, internal bargaining), and physical relapse (actual return to substance use, beginning with a lapse that can escalate rapidly). Relapse prevention interventions are most effective when directed at the emotional stage, before the cycle reaches the physical stage.
References
- National Institute on Drug Abuse. (2024). Treatment and Recovery. https://nida.nih.gov/publications/drugs-brains-behavior-science-addiction/treatment-recovery
- Substance Abuse and Mental Health Services Administration. (2023). Relapse Prevention. https://www.samhsa.gov/find-help/national-helpline
- American Psychiatric Association. (2022). Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR).
- National Institute on Drug Abuse. (2023). Opioid Overdose Crisis. https://nida.nih.gov/research-topics/opioids/opioid-overdose-crisis
- Marlatt, G.A., & Gordon, J.R. (1985). Relapse Prevention: Maintenance Strategies in the Treatment of Addictive Behaviors. Guilford Press.
- Witkiewitz, K., & Marlatt, G.A. (2004). Relapse prevention for alcohol and drug problems. American Psychologist, 59(4), 224–235.


