


Yes, wellbutrin is not an SSRI.
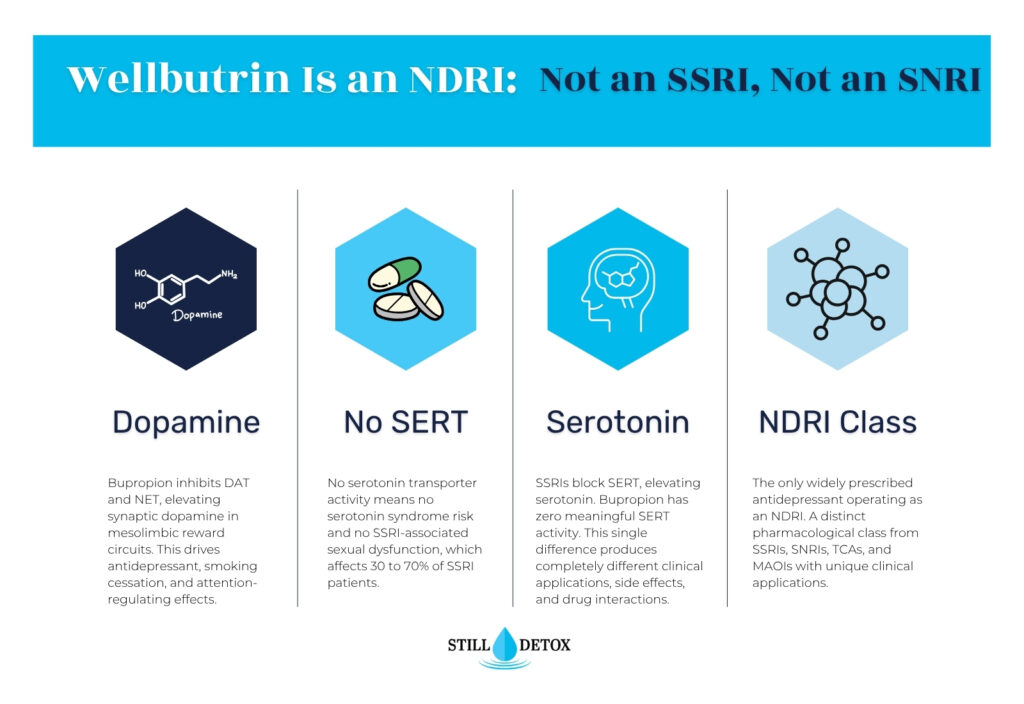
It is classified as a norepinephrine-dopamine reuptake inhibitor (NDRI), a pharmacologically distinct antidepressant class that targets the dopamine and norepinephrine transporters rather than the serotonin transporter that selective serotonin reuptake inhibitors block. This distinction produces entirely different side effect profiles, contraindications, drug interactions, and clinical applications.
Understanding what drug class Wellbutrin actually belongs to clarifies why it behaves so differently from SSRIs in practice, including its stimulant-like activation, lower sexual dysfunction rate, and documented misuse potential.
Key Takeaways
- Wellbutrin (bupropion) is a norepinephrine-dopamine reuptake inhibitor (NDRI), the only antidepressant in widespread clinical use belonging to this specific drug class.
- According to FDA prescribing data, Wellbutrin XL is approved for major depressive disorder and seasonal affective disorder; the same bupropion molecule marketed as Zyban carries FDA approval specifically for smoking cessation.
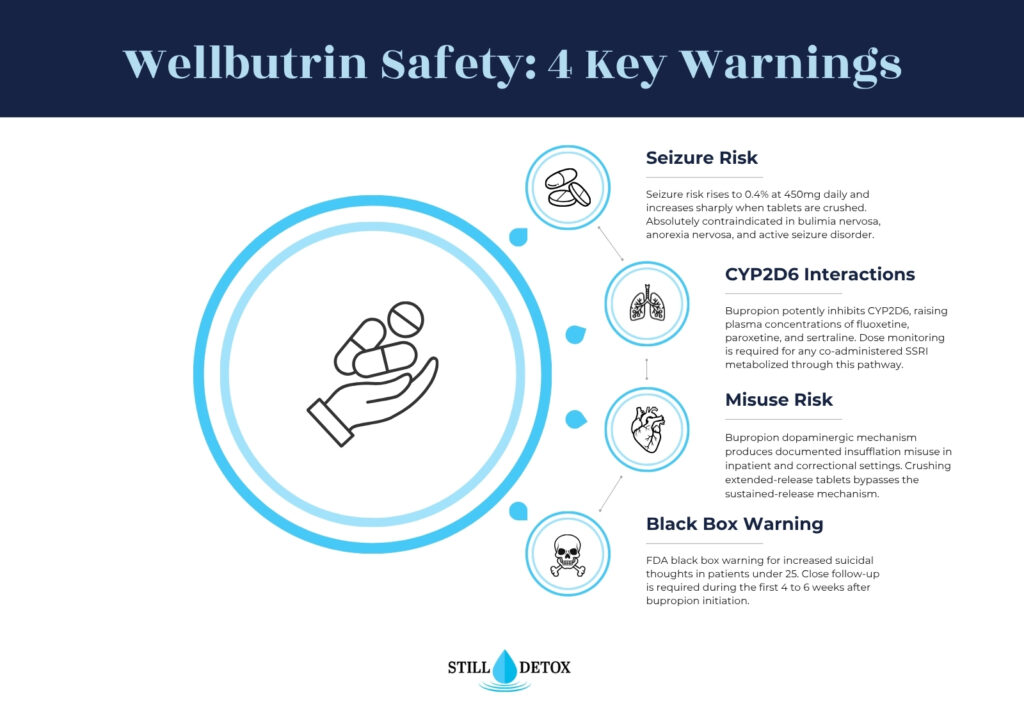
- Bupropion potently inhibits the CYP2D6 enzyme, creating clinically significant interactions with codeine, tramadol, and multiple psychiatric medications metabolized through this pathway.
- Unlike SSRIs, Wellbutrin produces no serotonin syndrome risk and does not typically cause serotonin-mediated sexual dysfunction or weight gain.
- According to a study in the Journal of Addiction Medicine, bupropion misuse through insufflation (snorting crushed extended-release tablets) has been documented in inpatient psychiatric and correctional settings.
What Is Wellbutrin?
Wellbutrin is the brand name for bupropion hydrochloride, a unicyclic aminoketone antidepressant belonging to the norepinephrine-dopamine reuptake inhibitor (NDRI) drug class. It is the only antidepressant in widespread clinical use that operates through this specific mechanism. Bupropion produces antidepressant, smoking cessation, and attention-regulating effects through dopaminergic and noradrenergic pathways entirely distinct from serotonergic antidepressant mechanisms.
Bupropion was first synthesized in 1969 and FDA-approved for depression in 1985. Initial market launch was suspended in 1986 after seizure reports during bulimia nervosa trials. It was relaunched in 1989 with modified dosing guidelines and an explicit contraindication against use in patients with eating disorders or seizure histories.
Wellbutrin Brand Names and Available Formulations
Available bupropion formulations include Wellbutrin IR (immediate-release, three times daily), Wellbutrin SR (sustained-release, twice daily), Wellbutrin XL (extended-release, once daily), and Aplenzin (bupropion hydrobromide, once daily). The smoking cessation formulation is marketed separately as Zyban at the same dose range as Wellbutrin SR. All formulations contain the same active molecule; release profile and dosing frequency differ while the pharmacological mechanism remains identical.
Forfivo XL is a 450mg extended-release formulation for patients requiring maximum therapeutic dosing. Generic bupropion is available at all release speeds and is bioequivalent to branded formulations. Some patients and clinicians report tolerability differences between immediate-release and extended-release versions due to peak plasma concentration differences.
FDA-Approved Uses for Bupropion
Wellbutrin XL is FDA-approved for major depressive disorder (MDD) and seasonal affective disorder (SAD). Zyban (bupropion SR) is FDA-approved as a smoking cessation aid. Evidence-supported off-label uses include attention-deficit/hyperactivity disorder (ADHD), antidepressant-induced sexual dysfunction reversal, bipolar depression adjunct therapy, and methamphetamine use disorder support.
Bupropion is not FDA-approved for anxiety disorders. Its lack of serotonergic activity makes it less effective than SSRIs or SNRIs for generalized anxiety disorder, panic disorder, and OCD as monotherapy. Prescribers treating comorbid depression and anxiety often combine bupropion with a low-dose SSRI rather than using bupropion alone.
How Does Wellbutrin Work?
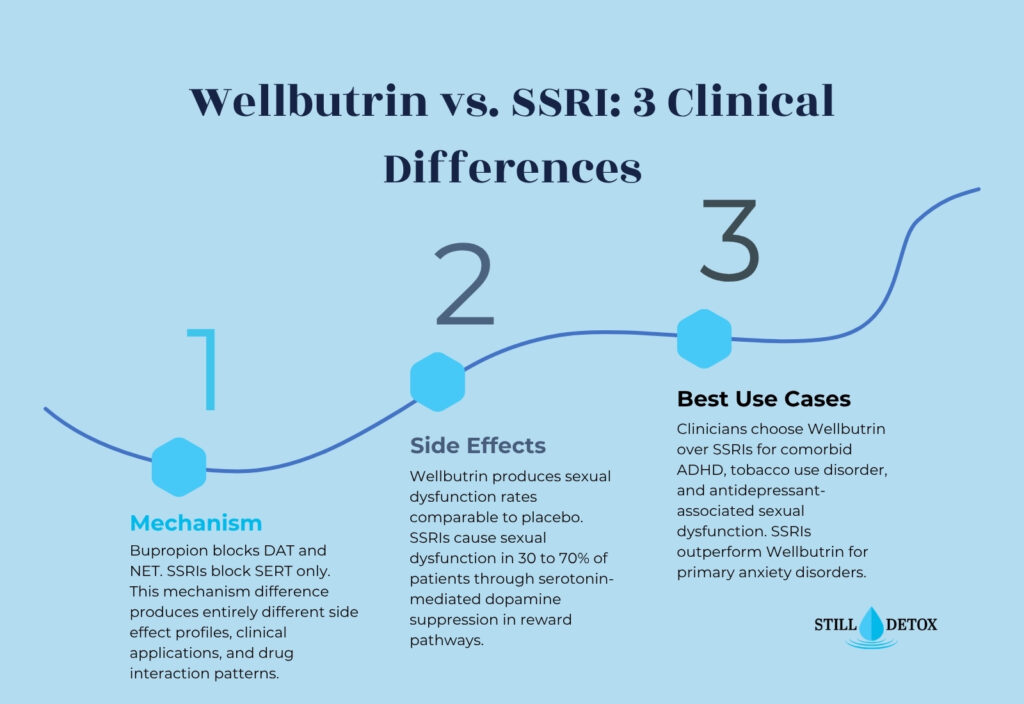
Wellbutrin blocks the dopamine transporter (DAT) and norepinephrine transporter (NET) at presynaptic terminals, preventing reuptake of both neurotransmitters after synaptic release. This dual DAT and NET inhibition elevates synaptic dopamine and norepinephrine concentrations without any significant action on the serotonin transporter (SERT) that defines SSRI pharmacology. The result is antidepressant efficacy through a completely separate neurotransmitter pathway.
NDRI Mechanism and Dopaminergic Effects
Bupropion binds the dopamine transporter (DAT) and norepinephrine transporter (NET), blocking presynaptic reuptake of both monoamines from the synapse. Elevated dopamine in the mesolimbic pathway produces bupropion’s activating and mild stimulant-like clinical effects. Elevated norepinephrine in prefrontal circuits supports executive function, attention, and antidepressant mood stabilization.
Bupropion’s dopaminergic activity also drives its smoking cessation mechanism. Nicotine dependence disrupts dopaminergic reward processing in the nucleus accumbens. Bupropion partially restores dopamine tone, reducing nicotine craving intensity. Additionally, bupropion antagonizes nicotinic acetylcholine receptors, blocking the reinforcing dopamine release that nicotine would otherwise trigger at these sites.
How Wellbutrin Differs from SSRIs Mechanically
SSRIs block the serotonin transporter (SERT), increasing synaptic serotonin concentrations across limbic, prefrontal, and brainstem circuits. Common SSRIs include fluoxetine (Prozac), sertraline (Zoloft), escitalopram (Lexapro), paroxetine (Paxil), and citalopram (Celexa). Meaningful antidepressant response typically requires 2 to 4 weeks of sustained SERT occupancy before clinical benefit emerges.
Wellbutrin does not block SERT, does not elevate synaptic serotonin, and produces none of the serotonergic side effects that define SSRI use. This explains why Wellbutrin does not cause serotonin syndrome, SSRI-associated sexual dysfunction, or serotonin-driven weight gain. It also explains why Wellbutrin is less effective than SSRIs as monotherapy for primary anxiety disorders mediated by serotonergic dysregulation.
Wellbutrin vs. Other Antidepressant Classes
Wellbutrin’s NDRI mechanism places it in a distinct pharmacological category from SSRIs, SNRIs, and MAOIs. Each antidepressant class targets different neurotransmitter systems with different clinical profiles, side effect spectrums, contraindications, and drug interaction risks. The comparison table below covers the four major antidepressant classes across the dimensions most clinically relevant to prescribing decisions.
| Feature | SSRI | NDRI (Wellbutrin) | SNRI | MAOI |
|---|---|---|---|---|
| Primary mechanism | SERT inhibition | DAT + NET inhibition | SERT + NET inhibition | MAO enzyme inhibition |
| Neurotransmitters elevated | Serotonin | Dopamine + norepinephrine | Serotonin + norepinephrine | All three monoamines |
| Common examples | Prozac, Zoloft, Lexapro | Wellbutrin, Zyban | Cymbalta, Effexor | Phenelzine, tranylcypromine |
| Sexual dysfunction rate | 30 to 70% | Comparable to placebo | Moderate to high | Moderate |
| Weight gain | Common | Neutral to mild loss | Common | Common |
| Seizure risk | Low | Dose-dependent (0.1 to 0.4%) | Low | Low |
| Serotonin syndrome risk | Yes (combinations) | No | Yes (combinations) | Yes (dietary + drug) |
| Discontinuation syndrome | Moderate to severe | Mild | Moderate to severe | Moderate |
| Activating vs. sedating | Mildly activating | Activating | Varies by agent | Varies by agent |
Wellbutrin vs. SSRIs: Key Clinical Differences
The most clinically significant difference between Wellbutrin and SSRIs is sexual function outcome. SSRIs produce sexual dysfunction in 30 to 70 percent of patients through serotonin-mediated suppression of dopaminergic reward signaling. Bupropion does not inhibit SERT and does not suppress dopamine in reward pathways, producing sexual dysfunction rates statistically comparable to placebo in controlled trials.
Wellbutrin is clinically preferred over SSRIs when antidepressant-associated sexual dysfunction represents a primary barrier to treatment adherence. It is also prescribed as an adjunct to SSRIs specifically to reverse SSRI-induced sexual side effects. Patients with comorbid ADHD, fatigue-dominant depression, or active tobacco use disorder often receive bupropion as a first-line choice over SSRI treatment.
Wellbutrin vs. SNRIs
SNRIs such as venlafaxine (Effexor) and duloxetine (Cymbalta) share bupropion’s norepinephrine reuptake inhibition but add serotonin transporter blockade. This dual mechanism makes SNRIs effective for anxiety disorders where bupropion is not. SNRIs produce higher rates of sexual dysfunction and more severe discontinuation syndrome than bupropion due to their SERT activity.
Bupropion’s dopamine transporter inhibition is absent from SNRIs, producing a distinct dopaminergic profile that SNRIs cannot replicate. Patients who do not respond to SSRI or SNRI treatment sometimes achieve response through bupropion’s NDRI mechanism. Combination bupropion plus SNRI therapy is used in treatment-resistant major depressive disorder under psychiatric supervision.
Can You Take Wellbutrin With an SSRI?
Combining bupropion with an SSRI is clinically practiced and evidence-supported for treatment-resistant major depressive disorder. Bupropion does not cause serotonin syndrome when combined with SSRIs because it produces no serotonergic agonism. However, bupropion potently inhibits CYP2D6, significantly increasing plasma concentrations of SSRIs metabolized through this pathway, including fluoxetine, paroxetine, and sertraline.
Combination therapy requires dose monitoring for SSRI toxicity secondary to CYP2D6 inhibition. Seizure threshold monitoring is required when combining bupropion with other seizure-lowering medications. Patients already prescribed alprazolam alongside an SSRI should have bupropion initiated cautiously due to layered CNS polypharmacy interaction risk.
Wellbutrin Side Effects and Safety Profile
Wellbutrin’s adverse effect spectrum differs substantially from SSRIs because the two drug classes operate through different neurotransmitter systems. Recognizing Wellbutrin’s distinct side effect profile helps clinicians and patients identify complications requiring medical intervention and make informed comparisons when choosing between antidepressant options.
Common Side Effects of Wellbutrin
Common Wellbutrin side effects affecting 5 to 30 percent of patients include:
- Insomnia and sleep disturbance from bupropion’s activating noradrenergic and dopaminergic stimulation of arousal circuits
- Dry mouth from reduced cholinergic activity and decreased salivary secretion
- Headache, most prominent during initial titration before neuroadaptation stabilizes
- Nausea, more common with immediate-release formulations due to higher peak plasma concentration fluctuations
- Agitation, restlessness, and increased anxiety from dopaminergic activation in limbic circuits
- Diaphoresis (increased sweating) from noradrenergic stimulation of eccrine gland secretion
These effects are dose-dependent and most pronounced during the first 2 to 4 weeks of treatment. Extended-release formulations (Wellbutrin XL) produce lower rates of nausea and agitation than immediate-release versions by reducing peak plasma concentration variability across the dosing interval.
Severe Side Effects and Safety Warnings
Seek medical evaluation immediately if any of the following occur during bupropion treatment:
- Seizure activity of any duration, including during initial dosing or after any dose increase regardless of prior tolerance
- Severe agitation, psychosis, or hallucinations indicating a bupropion-induced neuropsychiatric reaction
- Chest pain, hypertensive episode, or sustained tachycardia requiring cardiac assessment
- Allergic reactions including rash, angioedema, or urticaria indicating hypersensitivity
- New or worsening suicidal ideation per the FDA black box warning, especially in patients under 25 years old
Bupropion carries an FDA black box warning for increased suicidal thoughts in children, adolescents, and young adults aged 18 to 24 during initial antidepressant treatment. Seizure risk is dose-dependent: 0.1 percent at 300mg daily, rising to 0.4 percent at 450mg daily, and substantially higher when tablets are crushed, split, or misused.
Long-Term Risks and Contraindications
Bupropion is absolutely contraindicated in patients with current or prior seizure disorders, bulimia nervosa, and anorexia nervosa. Patients abruptly discontinuing alcohol face elevated seizure risk, and bupropion should not be initiated during active alcohol withdrawal without medical supervision. Unlike benzodiazepines, bupropion does not produce classical physical dependence at therapeutic doses.
Patients managing comorbid anxiety who are prescribed benzodiazepines such as clonazepam or alprazolam alongside bupropion require careful monitoring for CYP2D6-mediated benzodiazepine plasma concentration changes and for seizure threshold interactions. Long-term therapeutic bupropion use within its indicated contraindications is generally well-tolerated with no evidence of organ toxicity.
Wellbutrin Misuse and Abuse Potential
Bupropion’s dopamine transporter inhibition creates a misuse profile that is entirely absent from competitor articles on this topic and directly relevant to Still Detox’s clinical context. Bupropion is not a scheduled controlled substance and is not regulated as a drug of abuse at the federal level. However, its dopaminergic mechanism produces documented misuse in specific treatment and correctional populations.
Bupropion misuse occurs primarily through insufflation (crushing and snorting extended-release tablets), producing a rapid dopaminergic spike substantially higher than oral administration delivers. This mirrors insufflation misuse patterns documented for methylphenidate and other dopaminergic stimulant medications. Crushing extended-release tablets bypasses the sustained-release mechanism, delivering the full dose as an immediate bolus and dramatically elevating seizure risk.
Bupropion’s street nickname “poor man’s cocaine” reflects its dopaminergic mechanism and documented misuse potential in drug-experienced populations. Prescribers in addiction medicine contexts should evaluate misuse risk before initiating bupropion, monitor for tablet manipulation, early prescription refill requests, and requests for immediate-release over extended-release formulations.
Patients with stimulant use disorder histories who are also prescribed amphetamine salts for comorbid ADHD face additive seizure threshold reduction when bupropion is co-initiated. This combination requires careful risk-benefit assessment and ongoing dose optimization under psychiatric supervision.
Switching from an SSRI to Wellbutrin
Transitioning from an SSRI to bupropion requires a clinically managed protocol accounting for SSRI discontinuation syndrome, bupropion’s activation timeline, and CYP2D6 interaction dynamics during the overlap period. This transition guidance is absent from all three competing articles on this keyword.
Managing SSRI Discontinuation Before Starting Wellbutrin
SSRIs with longer half-lives, such as fluoxetine, tolerate more gradual tapering than shorter-acting agents like paroxetine and venlafaxine. Abrupt discontinuation of short-acting SSRIs produces discontinuation syndrome: dizziness, electric shock sensations (brain zaps), nausea, and rebound irritability from serotonin receptor hypersensitivity following loss of SERT occupancy.
Unlike gabapentin taper schedules that may require months of gradual reduction, most SSRI discontinuation is managed over 2 to 4 weeks under physician guidance. Cross-tapering, where bupropion is started at a low dose while the SSRI taper completes, is a common clinical strategy that reduces the depressive response gap between the two medications.
Managing the Transition Period
The SSRI-to-bupropion transition requires monitoring for three specific complications during the overlap period. First, bupropion’s CYP2D6 inhibition can raise residual SSRI plasma concentration during the taper, mimicking SSRI toxicity. Second, bupropion’s activating effects may temporarily worsen anxiety in patients who relied on SSRI anxiolytic activity. Third, a clinical response gap may temporarily intensify depressive symptoms before bupropion reaches therapeutic blood levels.
Patients should be informed that bupropion’s antidepressant onset requires 2 to 4 weeks of therapeutic dosing and that activating effects appear earlier than mood benefit. Patients with concurrent clonazepam dependence managed alongside antidepressant treatment require integrated dual-diagnosis medication planning during the transition period. Close follow-up during the first 4 to 6 weeks after bupropion initiation is standard of care to monitor seizure risk, psychiatric symptom trajectory, and functional status.
Dual Diagnosis Treatment and Wellbutrin at Still Detox
Bupropion is among the more commonly prescribed antidepressants in dual diagnosis treatment contexts, where major depressive disorder co-occurs with substance use disorder. Its dopaminergic mechanism supports mood restoration without producing serotonin syndrome risk or the SSRI-associated sexual dysfunction that reduces antidepressant adherence in substance use populations. Clinicians treating methamphetamine use disorder sometimes evaluate bupropion as an adjunct therapy given its shared dopaminergic mechanism.
Adults in South Florida managing depression alongside substance use disorder can access medically supervised dual diagnosis assessment and evidence-based treatment at Still Detox’s residential treatment program in the Boca Raton area. Same-day clinical assessments are available for individuals ready to begin treatment.
Frequently Asked Questions
Is Wellbutrin an SSRI?
No. Wellbutrin (bupropion) is a norepinephrine-dopamine reuptake inhibitor (NDRI), not an SSRI. It blocks the dopamine and norepinephrine transporters without meaningful activity at the serotonin transporter. SSRIs block the serotonin transporter selectively, producing entirely different clinical effects, side effect profiles, and contraindications. The two classes share antidepressant outcomes through distinct pharmacological mechanisms.
How is Wellbutrin different from SSRIs?
Wellbutrin elevates dopamine and norepinephrine without affecting serotonin. SSRIs elevate serotonin without significantly affecting dopamine. This produces distinct clinical profiles: Wellbutrin does not cause SSRI-associated sexual dysfunction, serotonin syndrome, or significant weight gain. Wellbutrin is more activating than most SSRIs and is more effective for comorbid ADHD and tobacco use disorder, while SSRIs outperform bupropion for primary anxiety disorders.
Is Wellbutrin a mood stabilizer or antidepressant?
Wellbutrin is an antidepressant, not a mood stabilizer. Mood stabilizers such as lithium, valproate, and lamotrigine work through different mechanisms to prevent manic and depressive cycling in bipolar disorder. Wellbutrin is FDA-approved for major depressive disorder and seasonal affective disorder. It can trigger manic episodes in undiagnosed bipolar patients and is typically prescribed cautiously or alongside a mood stabilizer in confirmed bipolar disorder.
Is Wellbutrin or Lexapro better?
Neither is universally better. Lexapro (escitalopram) is an SSRI with stronger evidence for generalized anxiety disorder and is often better tolerated in anxious patients. Wellbutrin performs better when SSRI-associated sexual dysfunction or weight gain is a primary concern, or when comorbid ADHD or tobacco use disorder is present. The choice depends on specific symptom profile, comorbid conditions, prior medication history, and individual tolerance to each drug’s side effects.
What is the biggest side effect of Wellbutrin?
Seizure risk is the most clinically significant safety concern with bupropion. At therapeutic doses up to 450mg daily, seizure risk is 0.1 to 0.4 percent. Risk increases substantially when tablets are crushed, when bupropion is combined with other seizure-threshold-lowering medications, or when used in patients with bulimia nervosa, anorexia nervosa, or prior seizure history. These risks produce bupropion’s most important absolute prescribing contraindications.
References
- U.S. Food and Drug Administration. (2017). Wellbutrin XL (bupropion hydrochloride extended-release tablets) prescribing information. https://www.fda.gov
- National Institute on Drug Abuse. (2021). Prescription stimulants DrugFacts. https://nida.nih.gov/publications/drugfacts/prescription-stimulants
- Stahl, S. M. (2021). Stahl’s essential psychopharmacology: Neuroscientific basis and practical application (5th ed.). Cambridge University Press.
- Clayton, A. H., Croft, H. A., & Handiwala, L. (2014). Antidepressants and sexual dysfunction: Mechanisms and clinical implications. Postgraduate Medicine, 126(2), 91–99.
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). American Psychiatric Publishing.
- Baribeau, D., & Araki, K. F. (2013). Intravenous bupropion: A previously undocumented method of abuse of a commonly prescribed antidepressant. Journal of Addiction Medicine, 7(3), 216–217.
- Stahl, S. M., Pradko, J. F., Haight, B. R., Modell, J. G., Rockett, C. B., & Learned-Coughlin, S. (2004). A review of the neuropharmacology of bupropion, a dual norepinephrine and dopamine reuptake inhibitor. Primary Care Companion to the Journal of Clinical Psychiatry, 6(4), 159–166.
- Jefferson, J. W., Pradko, J. F., & Muir, K. T. (2005). Bupropion for major depressive disorder: Pharmacokinetic and formulation considerations. Clinical Therapeutics, 27(11), 1685–1695.


