


Suboxone withdrawal lasts approximately one to four weeks for most people, with the most intense physical symptoms occurring in the first 72 hours after the last dose. Suboxone contains buprenorphine and naloxone, and because buprenorphine is a long-acting partial opioid agonist with a half-life of 24 to 42 hours, withdrawal onset is delayed, and its duration is longer than that of shorter-acting opioids.
Psychological symptoms of Suboxone withdrawal, including depression, anxiety, and cravings, can persist for weeks to months after physical symptoms resolve. The exact timeline depends on dose, duration of use, individual physiology, and whether the drug is stopped abruptly or tapered under medical supervision.
Key Highlights
- Suboxone withdrawal typically begins 24 to 72 hours after the last dose and peaks around days three to five, with physical symptoms generally resolving within one to two weeks.
- Buprenorphine has a half-life of up to 42 hours, making Suboxone withdrawal slower in onset and longer in duration than most opioid withdrawals, according to StatPearls (Shah and Huecker, 2023).
- Post-acute withdrawal syndrome (PAWS) affects a significant subset of patients, with psychological symptoms such as depression, insomnia, and cravings persisting for weeks to months beyond the acute phase.
- Subutex (buprenorphine only) and Zubsolv (buprenorphine/naloxone) produce withdrawal patterns nearly identical to Suboxone because all three share buprenorphine as the active opioid component.
- Medically supervised tapering with evidence-based adjunct medications significantly reduces withdrawal severity and duration compared to cold-turkey discontinuation.
What Is Suboxone and Why Does It Cause Withdrawal?
Suboxone is an FDA-approved prescription medication combining buprenorphine and naloxone, primarily used to treat opioid use disorder (OUD) as part of medication-assisted treatment (MAT). Buprenorphine is a partial opioid agonist that binds tightly to opioid receptors in the brain, suppressing withdrawal symptoms and cravings without producing the intense euphoria of full agonists like heroin or oxycodone.
Naloxone is included as an abuse deterrent and is poorly absorbed when taken as directed under the tongue. It activates only if the medication is injected, rapidly reversing any opioid effect and precipitating withdrawal in that scenario.
Because buprenorphine occupies opioid receptors continuously during treatment, the brain adapts its receptor activity and endorphin production downward over time. When Suboxone is stopped, the brain is left without adequate opioid receptor stimulation, and this neurochemical deficit produces the physical and psychological symptoms of withdrawal until the brain recalibrates on its own.
When Does Suboxone Withdrawal Start?
Suboxone withdrawal typically begins 24 to 72 hours after the last dose. This delayed onset is a direct consequence of buprenorphine’s long half-life of 24 to 42 hours, which means the drug clears from the body far more slowly than short-acting opioids like oxycodone, which has a half-life of only three to four hours.
In some individuals, particularly those on higher doses or those who have been on Suboxone for years, the onset of early withdrawal symptoms may be delayed further, appearing 48 to 72 hours after the last dose rather than within the first 24 hours.
For people tapering slowly under medical supervision, the transition is gradual, and the onset is significantly blunted. For those who stop abruptly, withdrawal symptoms can arrive suddenly and intensify rapidly over the first few days without any buffer period.
How Long Does Suboxone Withdrawal Last?
Suboxone withdrawal lasts between one and four weeks for the majority of patients when measured across its full acute phase. Physical symptoms are typically the most intense in the first week and diminish significantly by week two, while psychological symptoms follow a longer trajectory and may persist well into the second month or beyond.
The answer to how long Suboxone withdrawal lasts is highly individual and influenced by multiple clinical variables. A patient who has been on 2 mg per day for six months will have a meaningfully shorter withdrawal period than a patient who has been on 24 mg per day for five years.
Post-acute withdrawal syndrome (PAWS) extends the functional recovery period for many patients. PAWS involves persistent psychological and neurological symptoms, including low mood, anxiety, poor sleep, and difficulty experiencing pleasure, that continue after the acute physical withdrawal phase has resolved.
Suboxone Withdrawal Timeline: Phase by Phase
Hours 12 to 24: Onset
The earliest signs of Suboxone withdrawal are subtle and may initially resemble the onset of a flu. Patients begin to notice anxiety, restlessness, irritability, and mild muscle aches as buprenorphine levels drop below the threshold needed to suppress receptor activity. Yawning, a runny nose, and mild sweating are common first indicators that withdrawal has begun.
Days 1 to 3: Acute Phase Intensification
Physical symptoms escalate significantly during this period and represent the most physically uncomfortable stage of Suboxone withdrawal for most patients. Nausea, vomiting, diarrhea, abdominal cramping, fever, chills, sweating, muscle pain, and bone aches occur together during this phase. Blood pressure and heart rate can elevate, and insomnia becomes pronounced. Cravings for opioids or Suboxone itself intensify as the brain registers the absence of receptor stimulation.
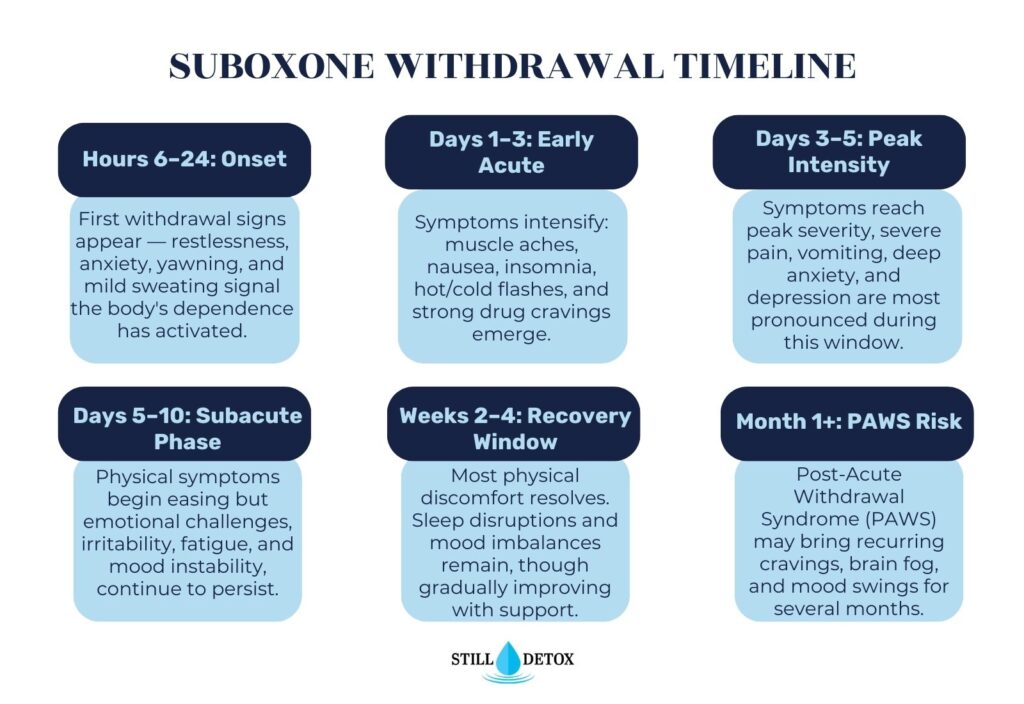
Days 3 to 5: Peak Intensity
Withdrawal symptoms reach their peak severity around days three to five for most patients stopping Suboxone abruptly. Physical symptoms are at their most overwhelming during this window, and psychological symptoms, including severe anxiety, depression, and drug cravings, are simultaneously at their strongest. This is clinically the highest-risk window for relapse, and medical supervision is most critical during these days.
Days 5 to 14: Gradual Resolution of Physical Symptoms
Physical symptoms begin declining in intensity after day five for most patients. Nausea, vomiting, and diarrhea typically improve first. Muscle aches become less severe but may persist at a lower level. Insomnia, fatigue, and mood instability often remain prominent during this period even as physical pain recedes. Cravings can remain intense and require active clinical management.
Weeks 2 to 4: Psychological Phase
By the second week, most acute physical symptoms have significantly resolved for patients who have not relapsed. Depression becomes the dominant symptom during this phase, as the brain’s natural endorphin system is still recalibrating. Motivation, emotional regulation, and cognitive function may feel impaired. Sleep quality often remains poor, with vivid or disturbing dreams being commonly reported during this period.
Beyond Week 4: Post-Acute Withdrawal Syndrome (PAWS)
A subset of patients experience post-acute withdrawal syndrome following the acute withdrawal phase. PAWS involves persistent and fluctuating psychological symptoms, including depression, anxiety, anhedonia (inability to feel pleasure), brain fog, irritability, and sleep disruption. These symptoms are not constant but tend to cycle unpredictably and can last weeks to months. PAWS significantly increases relapse risk and requires ongoing therapeutic and medical support beyond the initial detox period.
Suboxone Withdrawal Symptoms
Understanding the full symptom picture helps patients and families recognize what is clinically expected versus what requires emergency intervention.
Physical Symptoms of Suboxone withdrawal include:
- Nausea, vomiting, and diarrhea
- Muscle aches, bone pain, and body cramps
- Sweating, chills, and hot and cold flashes
- Fever and elevated heart rate
- Runny nose, watery eyes, and yawning
- Goosebumps and skin sensitivity
- Fatigue and severe lack of energy
- Headache and dizziness
Psychological Symptoms of Suboxone withdrawal include:
- Intense opioid cravings
- Anxiety and panic attacks
- Depression and feelings of hopelessness
- Irritability and anger
- Difficulty concentrating and brain fog
- Vivid or disturbing dreams
- Anhedonia (inability to feel pleasure from normal activities)
Sleep-Related Symptoms of Suboxone withdrawal include:
- Severe insomnia that persists beyond the acute phase
- Restless legs syndrome, particularly at night
- Hypersomnia (excessive sleepiness) during the day
- Fragmented, non-restorative sleep cycles
How Long Does Suboxone Insomnia Last?
Suboxone-related insomnia is one of the most persistently distressing symptoms of withdrawal and often outlasts other physical symptoms by several weeks. During the acute phase (days one through fourteen), insomnia is driven by neurological hyperactivation as the opioid system destabilizes. After acute symptoms resolve, insomnia frequently continues as a component of PAWS.
For many patients, sleep quality begins improving meaningfully around weeks three to four post-discontinuation, though full normalization can take two to three months in those with prolonged use histories. Restless legs syndrome, which disrupts sleep onset, is particularly common in the early withdrawal weeks and may require specific medical management.
Medical options for Suboxone withdrawal insomnia include clonidine, which reduces autonomic hyperactivation, trazodone for sleep maintenance, and melatonin for sleep onset. At Still Detox, sleep quality is assessed and managed as an independent clinical priority throughout the detox process, because untreated insomnia significantly increases relapse risk during recovery.
Subutex Withdrawal: Symptoms and Timeline
Subutex is the brand name for buprenorphine-only formulations, meaning it contains no naloxone. It is prescribed in specific clinical situations, including for patients who are allergic to naloxone or for pregnant individuals receiving medication-assisted treatment for opioid use disorder.
Because Subutex contains buprenorphine as its active ingredient, Subutex withdrawal symptoms and the Subutex withdrawal timeline are virtually identical to those of Suboxone. The same pharmacokinetics apply, including buprenorphine’s long half-life of 24 to 42 hours, which delays onset and extends the withdrawal period compared to short-acting opioids.
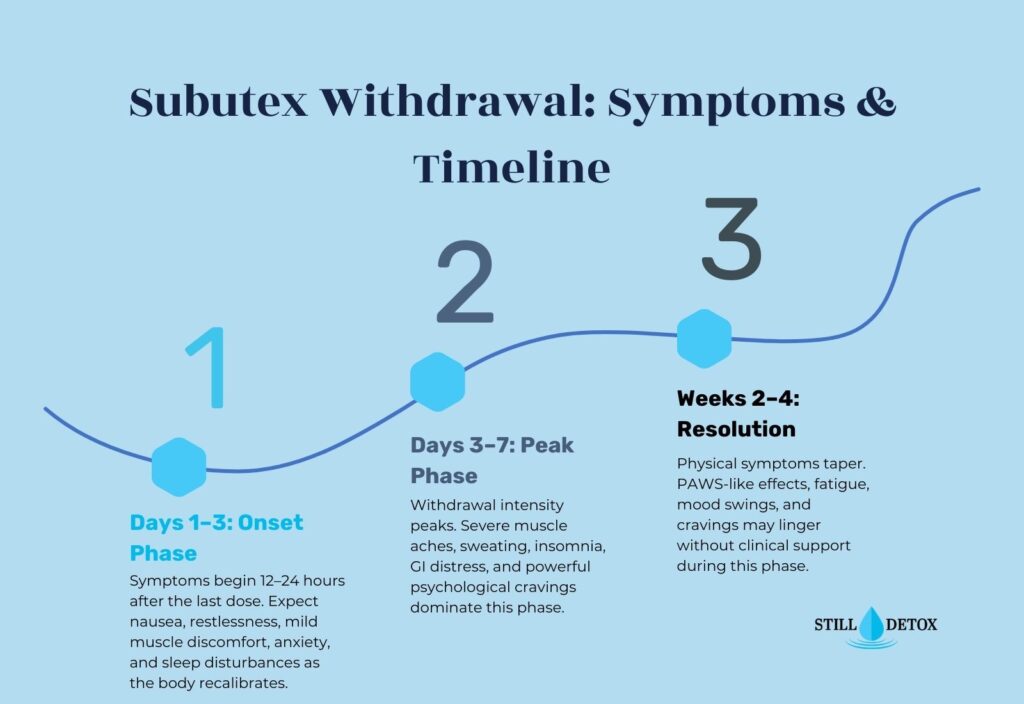
Subutex withdrawal begins 24 to 72 hours after the last dose, peaks around days three to five, and follows the same phase structure described above. Patients transitioning from Subutex to abstinence benefit from the same supervised tapering protocols used for Suboxone discontinuation, with gradual dose reductions over weeks to months, depending on the starting dose.
Zubsolv and Buprenorphine Withdrawal
Zubsolv is a brand-name buprenorphine and naloxone sublingual tablet, pharmacologically equivalent to Suboxone but formulated differently for improved absorption and taste. Because its active components are identical, Zubsolv withdrawal follows the same timeline and symptom profile as Suboxone withdrawal.
Generic buprenorphine products and other buprenorphine and naloxone formulations, including Bunavail and Cassipa, also produce the same withdrawal pattern when discontinued. The clinical management approach is consistent across all buprenorphine-containing formulations.
Patients switching from Zubsolv or generic buprenorphine treatment to a taper-to-discontinuation plan should work with a prescribing physician to design a dose reduction schedule tailored to their treatment history. Abrupt discontinuation of any buprenorphine product carries the same acute withdrawal risks as stopping Suboxone suddenly.
Factors That Affect How Long Suboxone Withdrawal Lasts
No two Suboxone withdrawal experiences are identical. Several clinical variables significantly influence both the severity and duration of withdrawal symptoms in individual patients.
The following are the factors that affect how long Suboxone withdrawal lasts:
- Dose and Duration of Use: Higher daily doses and longer treatment durations produce greater neuroreceptor adaptation, leading to more severe and prolonged withdrawal. A patient on 2 mg per day for three months will experience a markedly shorter and milder withdrawal than a patient on 24 mg per day for five years.
- Method of Discontinuation: Abrupt cessation produces the most severe and longest withdrawal. A structured medical taper, gradually reducing dose over weeks to months, allows the brain to adjust incrementally and significantly reduces both peak symptom severity and total withdrawal duration.
- Individual Physiology: Age, body weight, metabolic rate, and genetic variation in opioid receptor density all influence how the body processes and clears buprenorphine and how quickly the brain recalibrates after discontinuation.
- Co-occurring Mental Health Conditions: Patients with pre-existing depression, anxiety disorders, or PTSD typically experience more severe psychological symptoms during withdrawal and are at higher risk for PAWS. Integrated dual diagnosis treatment is essential for this population.
- Polydrug Use: Concurrent use of alcohol, benzodiazepines, or other opioids alongside Suboxone complicates the withdrawal process and may require a sequenced detox approach that addresses multiple substances simultaneously under medical supervision.
Is Suboxone Withdrawal Dangerous? Can You Die from It?
Suboxone withdrawal, while profoundly uncomfortable, is generally not directly fatal in otherwise healthy adults when managed properly. Unlike alcohol or benzodiazepine withdrawal, opioid withdrawal does not typically produce life-threatening seizures or cardiovascular collapse as a direct pharmacological consequence of the withdrawal process itself.
However, Suboxone withdrawal carries serious indirect risks that can become fatal without proper clinical oversight. The most significant danger is relapse. A patient who discontinues Suboxone and relapses to illicit opioid use faces extreme overdose risk because their opioid tolerance has dropped dramatically during abstinence. Using the same dose they used prior to Suboxone treatment can trigger respiratory depression and death.
Additional risk factors that increase the danger of Suboxone withdrawal include severe dehydration from vomiting and diarrhea, cardiovascular complications in patients with underlying heart disease, and suicidal ideation that can emerge during the depressive phase of withdrawal. These factors make medical supervision during Suboxone withdrawal not just preferable but clinically necessary for safe outcomes.
Suboxone Detox: Cold Turkey vs. Medical Taper
Stopping Suboxone cold turkey means discontinuing the medication abruptly without a dose reduction plan. Cold turkey discontinuation produces the most intense withdrawal symptoms, carries the highest risk of relapse, and provides no clinical buffer for the neurological adjustment the brain must undergo after long-term buprenorphine use.
A supervised inpatient medical detox is the evidence-based standard of care for Suboxone discontinuation. Tapering involves gradually reducing the daily dose in incremental steps over a physician-determined schedule, typically spanning several weeks to several months, depending on the starting dose and the patient’s clinical history. This approach gives the brain time to upregulate its endogenous opioid activity in a controlled manner.
During a medically supervised taper at Still Detox, patients receive adjunct medications to manage specific symptoms throughout the reduction process. These include clonidine for autonomic symptoms such as sweating and elevated blood pressure, anti-nausea medications, non-opioid sleep aids, and non-addictive medications for anxiety and mood support, as clinically indicated.
Medications Used to Manage Suboxone Withdrawal
Several FDA-approved and clinically validated medications help manage the symptoms of Suboxone withdrawal and improve patient comfort and outcomes during the detox process.
- Clonidine: An alpha-2 adrenergic agonist that reduces the nervous system hyperactivation responsible for sweating, elevated blood pressure, rapid heart rate, anxiety, and muscle cramps. Clonidine does not address cravings but meaningfully reduces physical distress during withdrawal.
- Lofexidine (Lucemyra): The first non-opioid medication specifically FDA-approved to treat opioid withdrawal symptoms in adults. Lofexidine works through a similar mechanism to clonidine and is approved for up to 14 days of use beginning within the first days of abstinence.
- Anti-nausea Medications: Ondansetron (Zofran) and promethazine are commonly used to manage nausea and vomiting during the acute phase, improving patient comfort and reducing the risk of dangerous dehydration.
- Antidepressants: SSRIs or SNRIs may be initiated during the withdrawal period for patients with co-occurring depressive disorders or for those experiencing severe psychological symptoms of PAWS.
- Non-opioid Sleep Aids: Trazodone, melatonin, and hydroxyzine can support sleep quality during withdrawal without addiction risk, addressing one of the most persistently disabling and relapse-driving symptoms of the process.
How to Safely Stop Taking Suboxone
Stopping Suboxone safely requires a physician-guided plan, adequate time, and integrated support that addresses both the physical and psychological dimensions of discontinuation.
The first step is a clinical evaluation by a prescribing physician or addiction medicine specialist to assess the appropriate tapering rate based on current dose, duration of use, and overall health. Self-directed tapering without medical oversight significantly increases the risk of severe symptoms and relapse.
At Still Detox, our medical team designs individualized Suboxone taper protocols for patients alongside full medical detox support. Cognitive Behavioral Therapy (CBT), individual counseling, group therapy, nutritional support, and peer recovery engagement are integrated with the medical taper to address all dimensions of recovery simultaneously. For patients with co-occurring alcohol, benzodiazepine, or stimulant use disorders, our dual diagnosis model sequences and manages all aspects of the detox process safely.
Frequently Asked Questions
How long does Suboxone withdrawal last?
Suboxone withdrawal typically lasts one to four weeks for acute physical symptoms, with psychological symptoms, including depression, anxiety, and cravings, potentially persisting for weeks to months as part of post-acute withdrawal syndrome. The exact duration depends on dose, duration of use, and whether the medication is tapered or stopped abruptly.
When does Suboxone withdrawal start?
Suboxone withdrawal typically begins 24 to 72 hours after the last dose, reflecting buprenorphine’s long half-life of 24 to 42 hours. Onset may be further delayed in patients on higher doses or those with slower metabolic clearance rates.
How long does Subutex withdrawal last?
Subutex withdrawal lasts approximately the same duration as Suboxone withdrawal, since both medications contain buprenorphine as the active opioid component. Symptoms begin 24 to 72 hours after the last dose and follow the same phase-based timeline, typically resolving acutely within one to two weeks with proper medical support.
Can you die from Suboxone withdrawal?
Suboxone withdrawal is not typically directly fatal in healthy adults, but it carries serious indirect risks, including relapse to illicit opioids at dramatically reduced tolerance, which creates extreme overdose and death risk. Medical supervision during withdrawal is essential to manage these dangers safely.
How long does Suboxone insomnia last?
Suboxone-related insomnia often persists beyond the acute withdrawal phase and may last two to three months in patients with long treatment histories. Sleep begins to normalize around weeks three to four for most patients, meaningfully, though restless legs and sleep fragmentation may require targeted medical management.
How long does suboxone detox last?
Acute suboxone detox, meaning the period of most intense physical symptoms, typically lasts five to ten days. A full medically supervised detox and stabilization period, including management of psychological symptoms and early recovery support, generally spans two to four weeks at a minimum.
What are the symptoms of Suboxone withdrawal?
Common Suboxone withdrawal symptoms include nausea, vomiting, diarrhea, muscle aches, sweating, chills, fever, insomnia, anxiety, depression, intense opioid cravings, irritability, and fatigue. Psychological symptoms typically persist longer than physical symptoms and require ongoing clinical and therapeutic management.
Is Suboxone withdrawal bad?
Suboxone withdrawal is considered more prolonged than many opioid withdrawals because of buprenorphine’s long half-life, though it is generally less acutely intense than withdrawal from heroin or fentanyl. Without medical support, it can be severely uncomfortable, and the risk of relapse is high, which is why supervised detox is strongly recommended.
How long do people stay on Suboxone?
Treatment duration varies significantly based on individual clinical need. SAMHSA guidelines support long-term and indefinite Suboxone maintenance for many patients because sustained medication-assisted treatment produces better outcomes than short-term use. Some patients taper off within six to twelve months, while others remain on maintenance therapy for several years. The decision to discontinue should always be made collaboratively with a prescribing physician based on stability, relapse risk, and overall recovery progress.
What is the 3-day rule with Suboxone?
The 3-day rule refers to the clinical requirement that a patient must be in mild to moderate opioid withdrawal, typically waiting at least 12 to 24 hours after their last short-acting opioid use or 24 to 72 hours after their last long-acting opioid use, before taking their first Suboxone dose. Starting Suboxone too early while full opioid agonists still occupy receptors can precipitate sudden, severe withdrawal. The three-day window is most commonly referenced in the context of transitioning from long-acting opioids such as methadone or fentanyl to buprenorphine treatment.
What is the new treatment for opioid addiction?
Buprenorphine-based medications, including Suboxone, remain the evidence-based standard of care, but several newer approaches have emerged. Extended-release injectable buprenorphine (Sublocade), administered monthly by a clinician, eliminates daily dosing and reduces diversion risk. Naltrexone (Vivitrol), as a monthly injection, is another non-opioid option for patients who have completed detox. Emerging research also supports low-dose buprenorphine induction protocols for patients transitioning from fentanyl, which reduce the risk of precipitated withdrawal during the induction phase.
References
- Shah, M., & Huecker, M. R. (2023). Opioid withdrawal. StatPearls Publishing.
- Shulman, M., Wai, J. M., & Nunes, E. V. (2019). Buprenorphine treatment for opioid use disorder: An overview. CNS Drugs, 33(6), 567-580.
- Kosten, T. R., & Baxter, L. E. (2019). Effective management of opioid withdrawal symptoms: A gateway to opioid dependence management. The American Journal on Addictions, 28(2), 55-62.
- Substance Abuse and Mental Health Services Administration. (2021). Medications for opioid use disorder: TIP 63. U.S. Department of Health and Human Services. https://store.samhsa.gov/product/tip-63-medications-opioid-use-disorder/PEP21-02-01-002
- Dydyk, A. M., Jain, N. K., & Gupta, M. (2023). Opioid use disorder. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK553166/
- U.S. Food and Drug Administration. (2023). Suboxone (buprenorphine and naloxone) sublingual film prescribing information. FDA. https://www.accessdata.fda.gov/drugsatfda_docs/label/2023/022410s042lbl.pdf
- Hallare, J., & Gerriets, V. (2023). Half life. StatPearls Publishing.
- American Society of Addiction Medicine. (2020). The ASAM national practice guideline for the treatment of opioid use disorder: 2020 focused update. ASAM.


