



No, medical consensus advises against taking Adderall during pregnancy.
Dextroamphetamine-amphetamine crosses the placenta and directly exposes the developing fetus to catecholamine stimulation, increasing the documented risk of premature birth, intrauterine growth restriction, fetal cardiac anomalies, and neonatal abstinence syndrome at birth. No federal agency has established a safe dose of Adderall during any trimester.
If you are currently prescribed Adderall and just confirmed a pregnancy, the answer depends on your trimester, your ADHD diagnosis status, and whether your prescribing clinician and OB-GYN have jointly evaluated your risk profile. Do not discontinue Adderall abruptly without prescriber guidance. This article presents the current evidence-based risk data so you can have an informed conversation with your medical team immediately.
Key Takeaways:
- Adderall (dextroamphetamine-amphetamine) carries an FDA Pregnancy Category C designation under the historical labeling system, meaning animal studies demonstrated fetal harm and no adequate controlled studies in pregnant humans exist.
- According to a landmark 2018 study by Huybrechts et al. in JAMA Psychiatry, first-trimester amphetamine exposure significantly elevates the risk of cardiac septal defects and gastroschisis compared to unexposed pregnancies.
- The search query “I took Adderall my entire pregnancy” has grown 77.5% year-over-year, reflecting widespread anxiety among pregnant patients about prior stimulant exposure, a concern this article directly addresses.
- Neonatal abstinence syndrome (NAS) develops in newborns whose fetal catecholamine systems were continuously stimulated by amphetamines in utero, producing tremors, feeding difficulties, and hyperirritability at birth.
- Non-pharmacological ADHD management including CBT adapted for adult ADHD, behavioral coaching, and environmental accommodations provides clinically meaningful symptom control without fetal exposure risk.
Is Adderall Safe During Pregnancy?
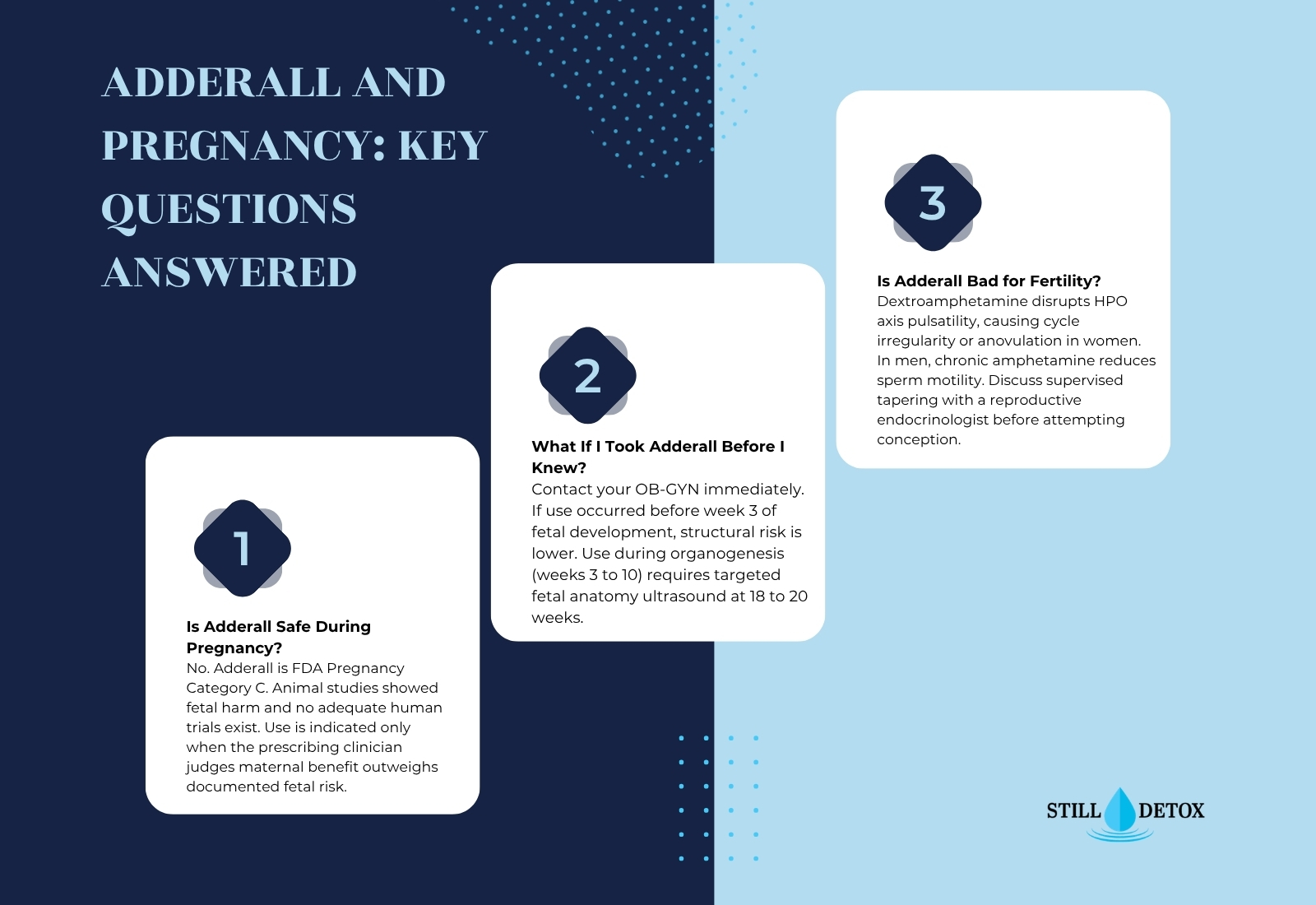
Adderall is not considered safe during pregnancy under current FDA prescribing information. The labeling designates it Pregnancy Category C, meaning available animal and limited human data do not support a safety assurance. Its use is indicated only when potential maternal benefit is judged to outweigh potential fetal risk by the prescribing clinician.
FDA Pregnancy Classification and Current Guidance
Adderall (dextroamphetamine-amphetamine) carries a historical FDA Pregnancy Category C classification, indicating that animal reproduction studies showed adverse fetal effects at drug-equivalent doses and no adequate, well-controlled human trials have established safety. Under the FDA’s updated Pregnancy and Lactation Labeling Rule (PLLR), which replaced the letter categories after 2015, the Adderall prescribing information now provides a narrative summary of available human and animal data.
The current prescribing information states that Adderall should be used during pregnancy only when the clinical benefit justifies the potential risk. Neonatal withdrawal is listed in the label as a documented risk in infants of mothers who took amphetamines during pregnancy, with the recommendation that these infants be observed for signs of neonatal abstinence syndrome.
How Adderall Crosses the Placenta
Dextroamphetamine crosses the placental barrier through passive diffusion driven by concentration gradients between maternal and fetal circulation. Once in fetal blood, dextroamphetamine binds to fetal adrenergic receptors and dopamine transporters identically to its action in adult tissue.
Placental catecholamine transfer from amphetamine exposure produces uterine vasoconstriction, reducing placental blood flow and restricting oxygen and nutrient delivery to the developing fetus. This uteroplacental insufficiency is the primary pathway through which Adderall use produces intrauterine growth restriction (IUGR) and prematurity in exposed pregnancies. Fetal catecholamine stimulation also elevates fetal heart rate and blood pressure, generating cardiovascular stress that the immature fetal cardiovascular system cannot adequately regulate.
How Adderall Affects Fetal Development
Adderall’s impact on fetal development depends on trimester, dose, and regularity of use, with first-trimester exposure carrying the highest risk for structural anomalies during the critical period of organogenesis.
First Trimester Risks
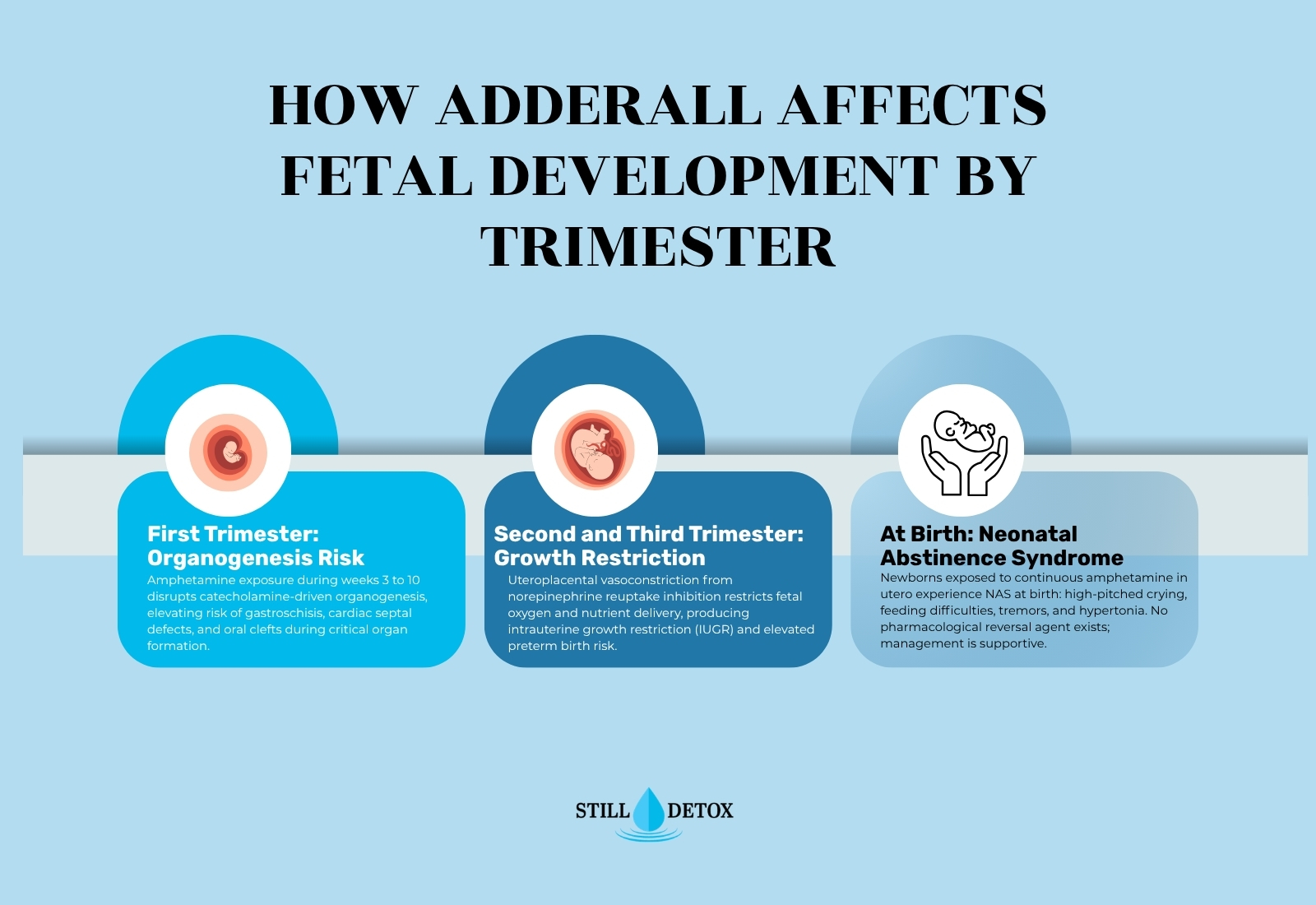
The first trimester encompasses organogenesis, the developmental window from approximately weeks 3 to 10 during which fetal organ systems differentiate from undifferentiated tissue. Amphetamine exposure during this window disrupts the catecholamine signaling that governs cell differentiation and morphogenesis of cardiac, gastrointestinal, and craniofacial structures.
First trimester Adderall exposure is associated with:
- Gastroschisis: A fetal abdominal wall defect in which intestines herniate outside the body at the umbilical ring; epidemiological studies consistently identify maternal amphetamine use as a risk factor
- Cardiac septal defects: Disruption of catecholamine-mediated cardiac morphogenesis elevates the incidence of ventricular and atrial septal defects in exposed fetuses, as documented in the Huybrechts 2018 JAMA Psychiatry cohort
- Oral clefts: A subset of epidemiological studies report a modest association between first-trimester amphetamine exposure and cleft palate, though the effect size is smaller than with anticonvulsant exposure
Second and Third Trimester Risks
After organogenesis concludes, the primary mechanisms of fetal harm from Adderall shift from structural disruption to uteroplacental compromise and direct catecholamine stimulation of fetal neural development during rapid cortical expansion.
Second and third trimester Adderall risks include:
- Intrauterine growth restriction (IUGR): Chronic uterine vasoconstriction from norepinephrine reuptake inhibition reduces oxygen and nutrient delivery, suppressing fetal growth velocity across the second and third trimesters
- Preterm birth: Stimulant-induced uterine muscle irritability increases the risk of spontaneous premature labor; preterm birth before 37 weeks is documented at significantly higher rates in amphetamine-exposed pregnancies
- Impaired fetal neurodevelopment: Catecholamine exposure during the third-trimester period of rapid dopaminergic and noradrenergic pathway maturation may disrupt the neural architecture underlying attention and executive function in the child
Neonatal Abstinence Syndrome at Birth
Neonatal abstinence syndrome (NAS) develops in newborns who were continuously exposed to amphetamines in utero and experience abrupt pharmacological discontinuation at birth. The newborn’s catecholamine and dopamine systems adapted to persistent fetal stimulation, and their removal triggers a withdrawal syndrome.
Amphetamine NAS produces symptoms within the first 24 to 72 hours of birth:
Amphetamine NAS clinical signs include:
- Neurological: High-pitched excessive crying, jitteriness, tremors, and increased muscle tone (hypertonia) that disrupts normal newborn movement and reflexes
- Feeding: Poor latch, ineffective suckling, and impaired hunger cuing that compromises neonatal weight gain and feeding establishment
- Sleep: Severely disrupted sleep-wake cycling inconsistent with normal newborn sleep patterns
Unlike opioid NAS, amphetamine NAS has no pharmacological reversal agent. Management is entirely supportive.
What If I Took Adderall Before I Knew I Was Pregnant?
If you took Adderall before confirming pregnancy, this is one of the most important conversations to initiate with your OB-GYN immediately, not an emergency, but urgent.
Most pregnancies are not confirmed until the 5th to 8th week of gestation. The high-risk organogenesis window runs from approximately weeks 3 to 10. If your Adderall use was limited to the period before implantation was confirmed and before week 3 of embryonic development, the structural anomaly risk window was not yet open. If use occurred during weeks 3 to 10 at prescription doses, your OB-GYN will likely recommend targeted fetal anatomy ultrasound at 18 to 20 weeks to screen for the cardiac and gastrointestinal anomalies associated with first-trimester amphetamine exposure.
Do not discontinue Adderall abruptly without prescriber guidance if you have a formal ADHD diagnosis. Untreated ADHD during pregnancy carries independent risks including impaired prenatal care adherence, heightened anxiety, and depression. The clinical decision requires individualized weighing of fetal exposure risk against the consequences of untreated maternal ADHD.
Is Adderall Bad for Getting Pregnant?
Adderall impairs fertility in both sexes through catecholamine-mediated disruption of reproductive hormonal signaling, making it a relevant clinical consideration before as well as during pregnancy.
In women, dextroamphetamine-amphetamine suppresses luteinizing hormone (LH) and follicle-stimulating hormone (FSH) pulsatility by disrupting hypothalamic-pituitary-ovarian (HPO) axis regulation. This hormonal suppression produces menstrual cycle irregularity and anovulatory cycles in a subset of women using stimulants regularly. In men, chronic amphetamine use reduces sperm motility and elevates the proportion of morphologically abnormal sperm, reducing fertilization probability.
Anyone trying to conceive who currently takes Adderall should discuss stimulant pharmacotherapy with their reproductive endocrinologist before beginning conception attempts. A full breakdown of how long Adderall stays in your system is relevant when planning the clearance period before conception.
Adderall While Trying to Get Pregnant
Individuals with diagnosed attention-deficit/hyperactivity disorder (ADHD) who take Adderall and are actively trying to conceive face a clinical decision that must not be made unilaterally or at the point of a positive pregnancy test.
The standard recommendation from reproductive endocrinologists and prescribing psychiatrists is to plan a supervised Adderall taper in the months preceding the intended conception window. Gradual discontinuation reduces fetal drug exposure during the highest-risk organogenesis period and avoids the clinical disruption of abrupt stimulant cessation in a patient with treated ADHD. For a detailed comparison of stimulant options and their pharmacokinetic differences relevant to this decision, the Vyvanse vs Adderall clinical overview covers key differences in drug structure, half-life, and misuse potential that prescribers weigh when evaluating alternatives during pregnancy planning.
Safer ADHD Alternatives During Pregnancy
No ADHD medication currently holds FDA approval with a demonstrated safety profile from controlled trials during pregnancy. Non-pharmacological management represents the first-line approach for most pregnant individuals with ADHD, with pharmacological alternatives reserved for cases where symptom severity creates an unacceptable clinical risk to the mother.
Non-Medication ADHD Management During Pregnancy
Non-pharmacological ADHD symptom management during pregnancy provides clinically meaningful benefit without any fetal pharmacological exposure:
Non-medication ADHD management options during pregnancy include:
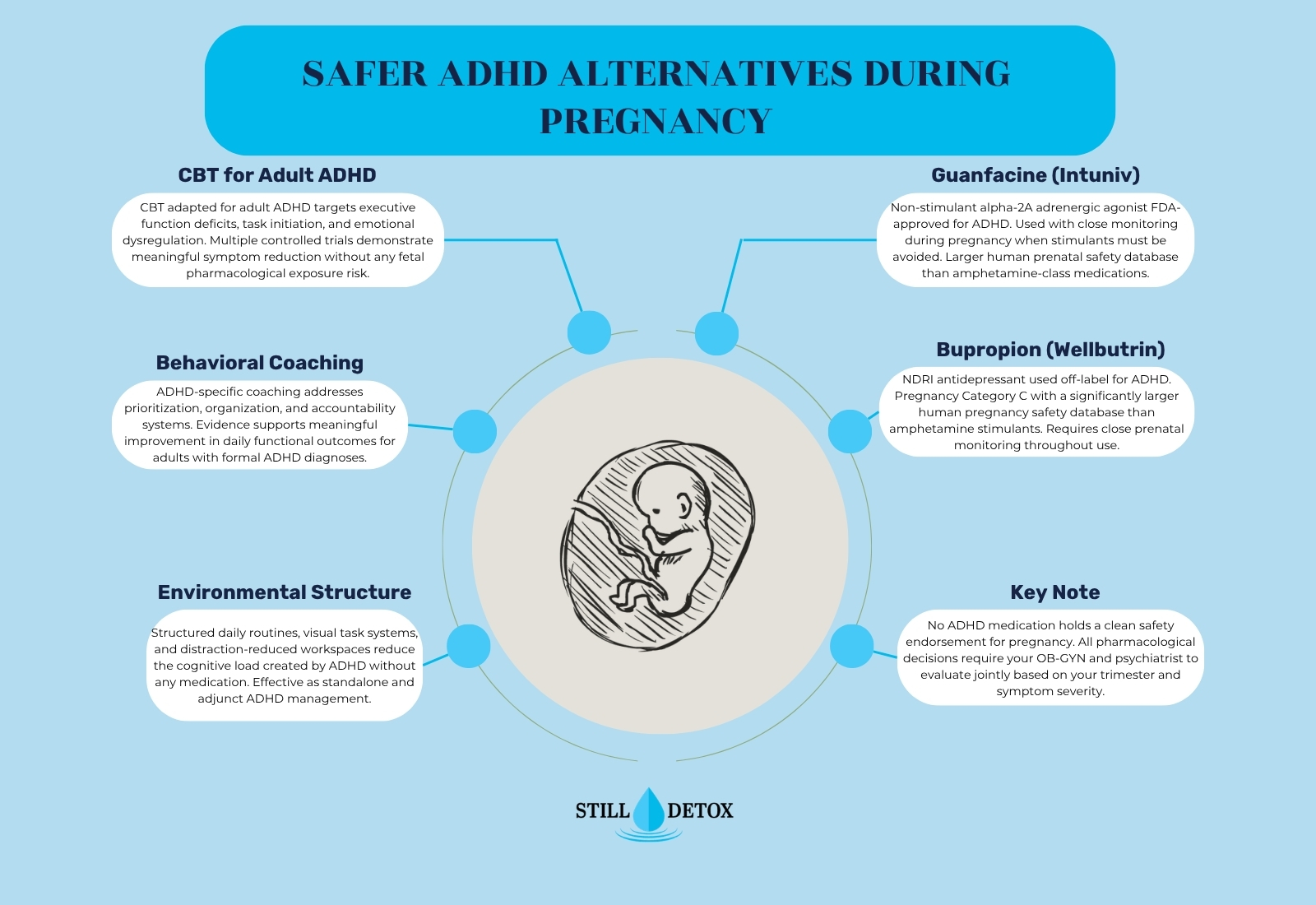
- CBT adapted for adult ADHD: Cognitive behavioral therapy targeting executive function deficits, task initiation, time management, and emotional dysregulation produces measurable symptom reduction in adults with diagnosed ADHD; multiple controlled trials support its efficacy
- Behavioral coaching: ADHD-specific coaching addresses organizational systems, prioritization, and accountability structures; demonstrates improvement in daily functional outcomes for adults with formal diagnoses
- Environmental accommodations: Structured daily routines, visual task management systems, distraction-reduced workspaces, and externalized reminder systems reduce the cognitive load created by ADHD without pharmacological risk
Medications With Lower Risk Profiles
When pharmacotherapy is clinically necessary during pregnancy, the following non-stimulant options carry larger or different human pregnancy safety databases than Adderall:
Lower-risk pharmacological options used cautiously during pregnancy include:
- Bupropion (Wellbutrin): A norepinephrine-dopamine reuptake inhibitor (NDRI) used off-label for ADHD; its human pregnancy safety database is substantially larger than stimulants due to widespread antidepressant use; classified Pregnancy Category C
- Guanfacine (Intuniv): A non-stimulant alpha-2A adrenergic agonist FDA-approved for ADHD; used with individual risk-benefit analysis in pregnancy, particularly in later trimesters when stimulant risks are highest
- Atomoxetine (Strattera): A selective norepinephrine reuptake inhibitor FDA-approved for ADHD; teratogenic effects have not been formally studied per current prescribing information, which limits confidence in safety claims
No medication on this list carries a clean safety endorsement for use during pregnancy. Every pharmacological decision during pregnancy requires direct individualized consultation with your OB-GYN and prescribing clinician.
What ADHD Medication Can You Take While Pregnant?
No ADHD medication has established safety in controlled human pregnancy trials. The clinical framework is individualized: weigh the severity of unmanaged ADHD symptoms against the specific medication’s known fetal risk profile and the trimester in which use would occur. Your OB-GYN and psychiatrist must make this decision jointly, with documentation of the clinical reasoning behind any pharmacological use during pregnancy.
Treatment at Still Detox
Still Detox in Boca Raton, Florida provides medically supervised care for stimulant use disorder, amphetamine dependence during and after pregnancy, and co-occurring conditions including untreated ADHD and prenatal anxiety. Same-day assessments are available.
Stimulant Use Disorder and Pregnancy
Individuals who cannot stop using Adderall during pregnancy despite genuinely wanting to may be experiencing stimulant use disorder as defined under DSM-5-TR, characterized by compulsive use producing clinically significant impairment despite serious medical and social consequences, including fetal risk. The amphetamine recovery program at Still Detox addresses compulsive stimulant use through evidence-based pharmacotherapy, CBT, and motivational interviewing. The medical detox program provides supervised discontinuation for patients requiring structured clinical support during stimulant withdrawal.
Dual Diagnosis Treatment
ADHD and stimulant use disorder frequently co-occur with major depressive disorder, prenatal anxiety, and trauma-related conditions that intensify during pregnancy and the postpartum period. The dual diagnosis treatment program at Still Detox delivers integrated psychiatric and addiction care, treating the substance use disorder and the underlying conditions driving it simultaneously.
Frequently Asked Questions
Can You Take Adderall While Pregnant?
No. Adderall is not considered safe during pregnancy. Dextroamphetamine-amphetamine crosses the placenta and directly exposes the fetus to catecholamine stimulation, increasing risks of intrauterine growth restriction, premature birth, cardiac defects, and neonatal abstinence syndrome. No dose of Adderall is established as safe during any trimester. If prescribed Adderall for ADHD, discuss tapering options and non-pharmacological alternatives with your prescribing clinician and OB-GYN immediately on confirming pregnancy.
What ADHD Medication Can You Take While Pregnant?
No ADHD medication holds an established safety record from controlled human pregnancy trials. Non-pharmacological management including CBT and behavioral coaching represents the lowest-risk first-line approach. When medication is clinically necessary, guanfacine and bupropion carry larger human pregnancy safety databases than stimulants and may be considered with careful monitoring. All decisions must be made jointly by your OB-GYN and prescribing clinician based on your specific trimester, symptom severity, and monitoring capacity.
What If I Took Adderall Before I Knew I Was Pregnant?
Contact your OB-GYN immediately to evaluate the timing and dose of your exposure. If use occurred before organogenesis began (before week 3 of embryonic development), structural anomaly risk is lower. Use during the 3 to 10-week organogenesis window warrants targeted fetal anatomy ultrasound at 18 to 20 weeks. Do not discontinue Adderall abruptly without prescriber guidance if you have a formal ADHD diagnosis that required pharmaceutical management.
Is Adderall Bad for Getting Pregnant?
Yes, Adderall can impair fertility in both sexes. Dextroamphetamine-amphetamine disrupts hypothalamic-pituitary-ovarian axis pulsatility in women, potentially causing cycle irregularity and anovulation. In men, chronic amphetamine use reduces sperm motility and concentration. Anyone using Adderall who is actively trying to conceive should discuss supervised tapering with a reproductive endocrinologist before beginning conception attempts, rather than discovering pregnancy while taking a daily stimulant during peak organogenesis risk.
Are There Alternatives to Adderall While Pregnant?
Yes. Non-pharmacological approaches including CBT for adult ADHD, behavioral coaching, and environmental structure reduce ADHD symptoms during pregnancy without fetal exposure risk. If medication is clinically necessary, non-stimulant options including guanfacine and bupropion carry larger human pregnancy safety databases than stimulants and may be considered with close monitoring. All pharmacological decisions require direct collaborative evaluation by your OB-GYN and prescribing psychiatrist based on your individual clinical situation.
Can You Take Adderall While Trying to Get Pregnant?
Adderall use during active conception attempts should be discussed with your prescriber and reproductive endocrinologist before attempting to conceive. Amphetamine disrupts HPO axis function and reduces sperm quality, potentially impairing fertility. The preferred approach is a supervised taper before the conception window so that Adderall has cleared your system before organogenesis begins, rather than discovering pregnancy while actively taking a daily stimulant.
References
- U.S. Food and Drug Administration. (2023). Adderall prescribing information. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/adderall-information
- National Institute on Drug Abuse. (2023). Prescription stimulants drug facts. National Institutes of Health. https://nida.nih.gov/publications/drugfacts/prescription-stimulants
- Substance Abuse and Mental Health Services Administration. (2024). 2023 National Survey on Drug Use and Health. https://www.samhsa.gov/data/release/2023-national-survey-drug-use-and-health-nsduh-releases
- Huybrechts, K. F., Broms, G., Christensen, L. B., et al. (2018). Association between methylphenidate and amphetamine use in pregnancy and risk of congenital malformations. JAMA Psychiatry, 75(2), 167–175.
- American Psychiatric Association. (2022). Diagnostic and statistical manual of mental disorders (5th ed., text rev.). DSM-5-TR. APA Publishing.


